

| Topic | Facial Trauma |
| Author | Orla Kelly |
| Duration | 1.5 hours |
Basics (20 mins)
Main session: (4 x 15 minute) case discussions covering the key points and evidence
Take home learning points: (5 mins)
Expectation is for the learners to have read the following links prior to the session:
https://dontforgetthebubbles.com/orbital-fractures/
https://dontforgetthebubbles.com/facial-bone-x-rays/
https://www.rch.org.au/trauma-service/manual/maxillofacial-injury/#toc-5
Some highly recommended optional extras:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4155887/
https://www.rcemlearning.co.uk/reference/zygomatic-and-nasal-injury/#1571914174387-f52a6ad5-3ffc
Basic Anatomy, Function and Initial Assessment

Above is a depiction of the adult facial bones. Paediatric anatomy differs slightly in the following ways, which affects the likelihood of fracture and injury pattern:
- Relative protrusion of the frontal bone from birth protects the smaller midface.
- Pneumatisation of the sinuses occurs in a stepwise fashion, leaving the facial bones more dense.
- The structure of bone means it is more elastic and resistant to fracture, but more prone to Greenstick fracture.
- The presence of unerupted permanent teeth adds strength to maxilla and mandible.
- Increased fat pads and soft tissue structures act as buffers to injury.
Facial fractures occur less commonly in children than in adults, and often follow a particular ‘top down’ pattern of injury in accordance with age. Due to the relative protrusion of the frontal bone from birth, younger children are more likely to have frontal bone and orbital floor fractures, with the incidence of nasal, zygomatic-maxillary complex and mandibular fractures becoming more common in later years, associated with play activities and sports. Nasal bone fractures are the most common fracture of childhood, followed by madibular, orbital, frontal skull and midface.
History
As with any trauma the history of the event is crucial. Facial fractures are often associated with significant intracranial or other injuries and a full history, primary and secondary survey are essential. History of the event will give an indication of the velocity of trauma and likelihood of other injuries. For instance – a direct blow to the orbit will increase suspicion of a blowout fracture rather than a fall from a bike.
In particular, do not forget:
- Red flag questions regarding head injury – loss of consciousness/vomiting/amnesia
- Occular symptoms – diplopia/change in visual acuity/pain on eye movements
- Jaw closing – does the patient feel their mouth closing is different?
A 12-year-old boy is brought into the department by his father. He was playing a rugby match and during a tackle, he received a blow to the face. When questioned, he thinks he was elbowed in the nose. He had epistaxis on the pitch which has since stopped.
What other questions would you like to ask regarding the history?
How would you examine this patient?
What investigations and management would be appropriate?
What other questions would you like to ask regarding the history?
It is important to treat facial injuries as head injuries and include any questions regarding head injury in your initial history. Delve further into the events surrounding the injury – how long did the epistaxis last? Was there any loss of consciousness, amnesia, or vomiting? If there are no red flags that warrant a CT scan, be sure to screen for concussion, and give written advice regarding cognitive rest and gradual return to school and sports if necessary.
How would you examine this patient?
On examination – visually inspect the face and nose looking for deformity and asymmetry. Ask regarding the previous appearance of the nose (not all deformities are acute!). Any saddle nose deformity or telecanthus warrants investigation for naso-orbital-ethmoidal fracture. Look closely at the orbits – assessing for conjunctival haemorrhage, panda eyes, pupillary reflexes, and eye movements. Check visual acuity, and visual fields and ask about diplopia. Visually inspect the nasal cavity looking for active epistaxis, septal deviation, and septal haematoma. Ask the patient to occlude one nostril and breathe through the other on each side. Ask the patient to open their mouth – look for posterior epistaxis or oral trauma.
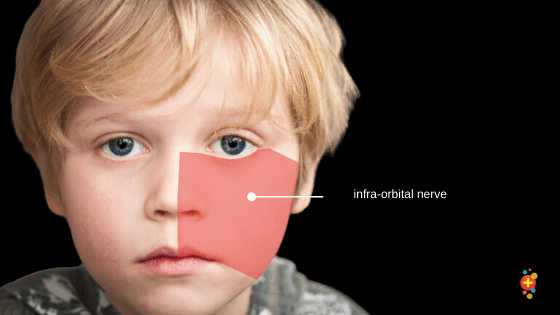
Palpate the facial bones laterally to medially (any possibility of pain should be kept until last – that way you stay friends longer) feeling for pinpoint tenderness or a step. Assess the sensation of the infraorbital nerve.
What investigations and management would be appropriate?
If the history and examination are consistent with a nasal bone fracture, there is no need for further imaging. Any septal haematoma must be urgently evacuated to avoid necrosis of the septum and resultant deformity. The patient should be discussed with local Max-Fax / ENT services and provided with a clinic appointment for the near future for possible closed reduction and external fixation if necessary.
Have a look at this video hosted by NEJM demonstrating nasal septal haematoma drainage.
A 6-year-old girl is brought in by ambulance after falling off her bike. She has been crying uncontrollably since. The fall was witnessed, she did not lose consciousness and has not vomited. She is holding the left side of her face. Mum reports there was no blood at the scene.
What is your first action in the management of this patient?
What clinical signs might give you a clue that a mandible fracture was present?
How would you investigate this injury?
What nerve can be damaged in this injury?
What follow-up is required?
What is your first action in the management of this patient?
All patients should be managed from an ABCDE approach. This girl has a patent airway and no respiratory or cardiovascular compromise. Her most immediate concern currently is pain which must be addressed before the examination is attempted. Oral ibuprofen and oral or rectal paracetamol can be used, but if the patient is in apparently acute severe pain, intranasal fentanyl can be used as an adjunct which will give immediate relief. Check out this post on analgesia in paediatrics.
After the patient has been given adequate analgesia, examination reveals no obvious facial deformity or bruising, but she is unwilling to open her mouth more than a few millimetres. She flinches when any attempt is made to palpate the left side of her jaw. You suspect a mandible injury.
Mandibular fractures are more common in children than in adults due to the ratio of medullary bone surrounded by thin cortical bone. Unlike adults which subscribe to the polo mint rule – that there must be two fracture sites – they can only have one. Condylar fractures are the most common, of which approximately 20% are bilateral. Of all mandible fractures, condylar fractures pose the highest risk of growth disturbance and joint hypermobility.
Always assess patients with facial trauma for other injuries (75% of mandibular fractures in children have other injuries) and pay particular attention to the cervical spine.

What clinical signs might give you a clue that a mandible fracture was present?
Other signs that indicate mandibular fractures include gingival wounds, mobile teeth segments, buccal or sublingual haematoma, and bleeding from the auditory canal with condylar fractures.
How would you investigate this injury?
Mandibular imaging usually consists of an OPG and a PA mandible. However, for uncooperative patients, lateral views or a CT scan may be required. CT scan may also be required to assess for TMJ dislocation or comminuted fractures.
Take a look at this DFTB post on mandible x-ray interpretation.
What nerve can be damaged in this injury?
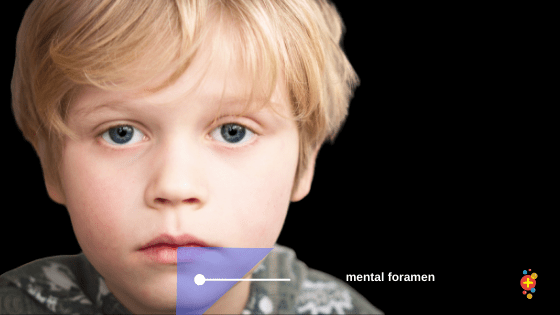
The inferior alveolar nerve can be damaged in mandibular injuries which travels adjacent to the lingual cortical surface on the inferior border of the mandible. Its branch the mental nerve exits the mental foramen and provides sensation to the chin and lower lip.
What follow up is required?
This patient must be discussed with on-call Max Fax colleagues. Often paediatric mandibular fractures are treated conservatively, however, if there is any blocking movement of the jaw then open fixation is required.
Read more about these injuries, including mandibular dislocations, in this DFTB post on mandibular injuries.
An 8-year-old boy is brought into the ED following a blow to the right eye when playing tennis. He is complaining of pain and has been vomiting.
Describe the anatomy of the orbit
What investigations are appropriate in this case?
Why is this patient vomiting, and what other signs or symptoms might you expect?
If the patient started complaining of severe pain in the affected eye, what might you consider?
Describe the anatomy of the orbit
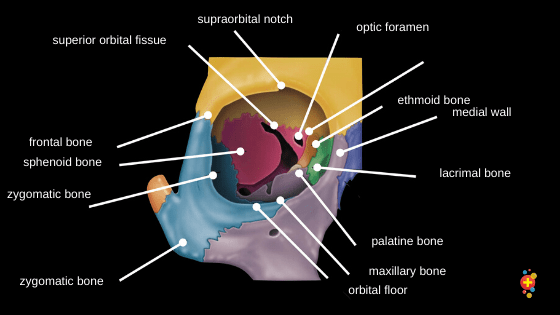
The orbit is a complex structure that is pyramidal in shape. In young children, due to the prominence of the frontal bone which bears the brunt of most trauma, the roof is more likely to be fractured. With direct trauma to the orbit, the globe is less likely to rupture than the floor is to fracture.
It is imperative to assess the conjunctiva, visual acuity, pupillary reflexes, visual fields, eye movements, and sensation of infraorbital nerve. Beware of the ‘white eye’ blowout fracture which is when there is no obvious globe injury, however, there is limited or no movement on upward gaze. An orbital blowout fracture can cause a trapdoor effect, where soft tissue has been trapped by the movement of the orbital floor. This injury requires urgent surgical intervention and discussion with Max Fax and Ophthalmology.
What investigations are appropriate in this case?
With an abnormal examination and a vomiting patient, it is reasonable to forego facial x-rays in favour of CT to avoid unnecessary radiation. The sign to look out for on X-ray of orbital fracture is the teardrop sign which is herniated muscle or fat visible at the roof of the maxillary sinus, and the black eyebrow sign, which signifies orbital emphysema, usually a medial fracture through to the ethmoid sinus.
Why is this patient vomiting, and what other signs or symptoms might you expect?
The oculo-cardiac reflex could be the cause of this child’s vomiting. It is mediated by connections between the ophthalmic branch of the trigeminal nerve and the vagus nerve. It can be associated with haemodynamic instability, hypotension, and bradycardia. It is yet another reminder of why we proceed with the ABC assessment of all patients in the first instance. Another cause could be rising intracranial pressure, and a CT brain is warranted. Early discussion with ophthalmology is essential, sometimes (not in the case of haemodynamic instability caused by the oculo-cardiac reflex) surgery is delayed for steroid therapy to prevent further optic nerve damage.
If the patient started complaining of severe pain in the affected eye, what might you consider?
Severe pain in an eye injury can be indicative of a retrobulbar haematoma. This causes increased pressure resulting in proptosis, blurred vision and an afferent pupillary defect. The only treatment is urgent lateral canthotomy. Have a look at this video from EM:RAP on how to perform a lateral canthotomy.
Read more about orbital fractures in this DFTB post.
A 12-year-old boy is brought in by ambulance following a road traffic accident. He was a pedestrian hit by a car moving at approximately 40km/hr. His GCS is 14 and he has obvious severe bleeding facial injuries.
Outline the initial management and stabilisation of this patient
What does Le Fort mean?
What are the next steps required for this patient?
Outline the management and stabilisation of this patient.
This case is one that should follow strict trauma life support protocols, and the candidates should be careful not to be distracted by obvious injuries. In the first instance, a trauma call should be made.
This patient should be immobilised with c-spine precautions. The presence of severe facial injuries is concerning regarding his airway. Lying flat with bleeding wounds increases the risk of aspiration and airway occlusion. His airway should be assessed for blood/teeth / debris and suctioned if necessary.
Head tilt is inappropriate due to the spinal precaution, and so jaw thrust would be the airway manoeuvre needed to maintain a patent airway. In this case, early intubation would be appropriate due to airway compromise and patient distress. After the airway is secured the rest of the ABC primary survey can be completed, including trauma imaging and advanced surgical skills as required. Children are at increased risk of hypothermia and haemodynamic instability in trauma and must be constantly reassessed.
These two #DFTB19 talks are definitely worth signposting:
Taking your trauma team to the next level: Anna Dobbie
Maturing your approach to trauma: Anne Weaver
No thoracic, abdominal, pelvic, or long bone injuries are detected during the child’s primary survey. Imaging of the brain, c-spine, and facial bones show a frontal subdural haematoma, a Le Fort II fracture, and fractured C4.
What does Le Fort mean?
Maxillary fractures are classified according to the Le Fort classification system.
- Le Fort I: A horizontal fracture through the floor of maxillary sinuses with the teeth contained within the detached fragment. Only palate moves.
- Le Fort II: A fracture which can be one-sided or bilateral fracture through the maxilla extending into the floor of the orbit, the nasal cavity and hard palate. This results in a pyramidal shaped fracture.
- Le Fort III: A fracture through the orbits in which the entire maxilla and one or more facial bones, the entire midface, becomes separated from the base of the skull. This is called craniofacial disjunction.

What are the next steps required for this patient?
This patient naturally requires discussion with neurosurgical services, orthopaediacs, and maxillofacial surgeons. His c-spine must remain protected and he is likely to require the evacuation of the frontal subdural. He also requires a thorough secondary survey. In this case, one of the mainstays of treatment is to prevent secondary brain injury.
He should be lying at a 30-degree tilt (still in spinal precautions), his temperature, glucose, and end-tidal CO2 should be kept in tight parameters, and an anticonvulsant should be given if there’s concern that he might have a seizure. Neurosurgery may request mannitol or hypertonic saline depending on scan results.
He should also receive tetanus cover and antibiotics for open facial fractures.
For further reading about neuroprotection in traumatic brain injuries, have a look at this Paediatric FOAM post.
Read more about maxillary fractures in this DFTB post.
A 14-year-old girl is brought in by ambulance following a sporting accident. She was playing camogie* without a helmet and was struck with a hurl (similar to a hockey stick) during a mid-air challenge. She received good pre-hospital analgesia by paramedics and is now comfortable. She has significant bruising and a laceration on the left side of her face. You suspect a zygomatic maxillary complex fracture.
*an Irish sport, sort of the female version of hurling (both Gaelic sports)
What specific injury pattern would you expect in a zygomatic maxillary complex (ZMC) fracture?
What neurological defects might be present?
What investigations are necessary?
What treatment should be instigated in the ED?
What specific injury pattern would you expect in a zygomatic maxillary complex (ZMC) fracture?
Facial injuries require a full examination from all sides; look for facial flattening from a bird’s eye view and enophthalmos from a worm’s eye view. Ipsilateral epistaxis can be severe; remember to check the back of the throat for a posterior bleed (this also helpfully assesses movement of the mandible). As always inspect the eye, and look for subconjunctival haemorrhage with no lateral border.
What neurological defects might be present?
Any patient with a suspected ZMC fracture requires a full and thorough cranial nerve examination. The sensory branches of cranial nerve V2 (infraorbital, zygomaticofacial, and zygomaticofrontal) all run in close proximity to the zygoma and can be damaged easily. This results in numbness of the cheek, upper lip, nose, and maxillary dentition if the infraorbital nerve is damaged (usually where it exits the infraorbital foramen), and numbness of the lateral cheek and anterior temporal area if the zygomaticofacial or zygomaticofrontal nerves are damaged (usually where they exit the zygoma by their eponymous foramina). If the fracture is severe, it can damage the facial nerve as it crosses superficial to the arch resulting in an ipsilateral facial palsy.
What investigations are necessary?
Facial xrays can show these fractures, but a CT is the gold standard, particularly if there is any obvious deformity or neurological deficit which will require operative management.
What treatment should be instigated in the ED?
This patient should receive tetanus and antibiotics given it is an open fracture. Some ZMC fractures in children are treated conservatively with decongestants and antibiotics (they are often greenstick with no great cosmetic or neurological sequelae), however, others require careful operative management, with the goals of treatment to restore form and function, without compromising future bone growth. Discussion with max fax on call is required. The patient should be advised against nose blowing in the interim!
Read more about zygomatic complex fractures in this DFTB post.

Question 1
A patient with a mandibular fracture may also complain of:
A. Loss of taste
B. Tingling or loss of sensation of the upper lip
C. Trismus
D. Tingling or loss of sensation of the lower lip and chin
Answer 1
The correct answer is D.
Due to damage to the inferior alveolar nerve as it exits the mental foramen.
Question 2
A patient with an obvious deformity to their left zygomatic arch also appears to have a facial droop. This is due to damage of what structure?
A. Cranial nerve V
B. Cranial nerve VI
C. Cranial nerve VII
D. Infraorbital nerve
Answer 2
The correct answer is C.
The facial nerve can be damaged in extreme cases of facial trauma, leading to paralysis of the ipsilateral facial muscles.
Question 3
A blowout fracture will cause the inability of:
A. Lateral gaze
B. Upward gaze
C. Medial gaze
D. Inferior gaze
Answer 3
The correct answer is B.
Due to entrapment of the inferior rectus muscle.
Question 4
Which of the following would require emergent intervention in a nasal fracture?
A. Dorsal swelling
B. Septal deviation
C. Septal haematoma
D. Loss of sense of smell
Answer 4
The correct answer is C.
Before septal necrosis develops.
Question 5
Open fractures require:
A. IV antibiotics
B. Tetanus status assessment
C. Thorough washout
D. All of the above
Answer 5
The correct answer is D – All of the above.
Question 6
Which of these is NOT part of the conservative management of a ZMC fracture?
A. Avoidance of nose blowing
B. Soft diet
C. Prophylactic antibiotics
D. Nasal decongestants
Answer 6
The correct answer is B.
Question 7
Which fractures of the mandible pose the highest risk of growth disturbance and joint hypomobility?
A. Condyle
B. Body
C. Angle
D. Ramus
Answer 7
The correct answer is A.












