

Assessing capillary refill time to identify shock has been ingrained in anyone who has taken one of the paediatric alphabet courses (APLS/PALS/PLS, etc.)—but how useful is it really?
Back to the beginning
As with most things in modern medicine, war breeds progress. In 1947, Henry Beecher and colleagues proposed capillary refill time (CRT) to determine the shock state. They allied ‘normal‘, ‘definite slowing‘ and ‘very sluggish‘ refill with ‘no’, ‘slight to moderate’ and ‘severe shock. This theory was based on just over 100 patients. As it entered common usage, initially for the assessment of trauma, an arbitrary value of normal being less than 2 seconds came into use.
Some basic pathophysiology
The use of capillary refill time as a surrogate marker for assessing shock or hydration status is underpinned by basic physiological principles. In shocked or dehydrated states, the peripheral vasculature undergoes vasoconstriction. This preserves blood flow to the vital organs – the brain, heart and kidneys – at the expense of less vital tissues. As systemic vascular resistance increases, the skin becomes cool and pale, with weak pulses; capillary refill time is prolonged.
How should you measure capillary refill time?
In the original literature, there was little agreement on how to measure CRT. Some papers suggest pressing on the nail bed of the right thumb for five seconds and then calculating refill using your pocket watch, whilst others use the sternum and a digital stopwatch. Very few of us, in practice, get out a watch to measure CRT, and in the current ‘bare below the elbows’ climate, many of us may not wear a watch at all.
And why do we press for five seconds, not ten or thirty? Is a longer compression time more accurate? Perhaps the true value in measuring CRT is that it provides a cognitive stop point in managing a sick child—five seconds to get our breathing under control—before proceeding. Data suggest that pressing for longer yields a longer CRT (by up to 1.4 seconds), but the results are inconsistent.
Where should you measure capillary refill time?
Does it matter if it is measured centrally (cCRT) on the sternum or peripherally (pCRT) on the nailbed? Common sense would suggest that there should be a discrepancy between the two purely due to distance. Several studies have borne this out.
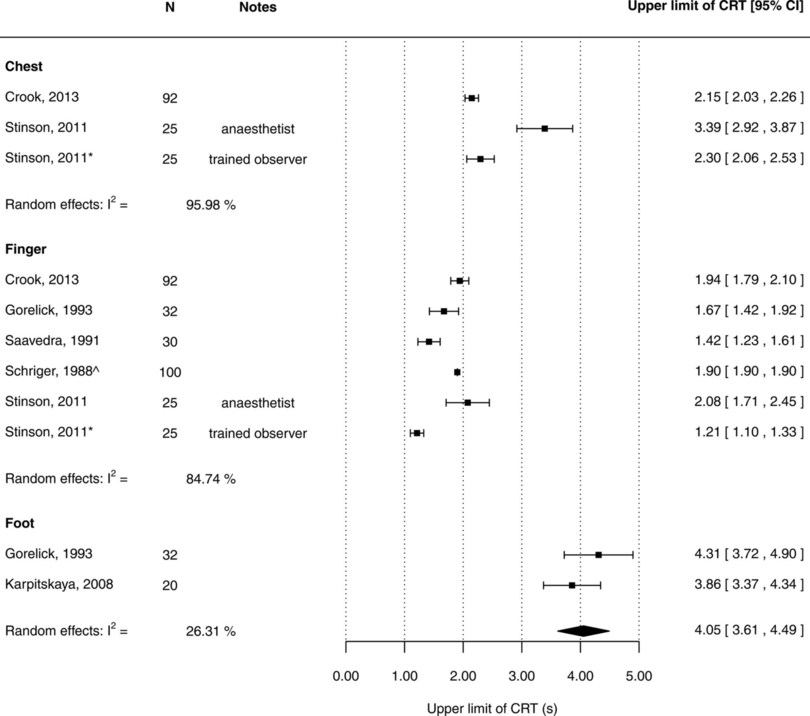
A 2014 systematic review by Fleming et al. found that, in children older than 7 days, the upper limit of normal CRT is 2 seconds when measured in the hands but 4 seconds when measured on the chest or foot.
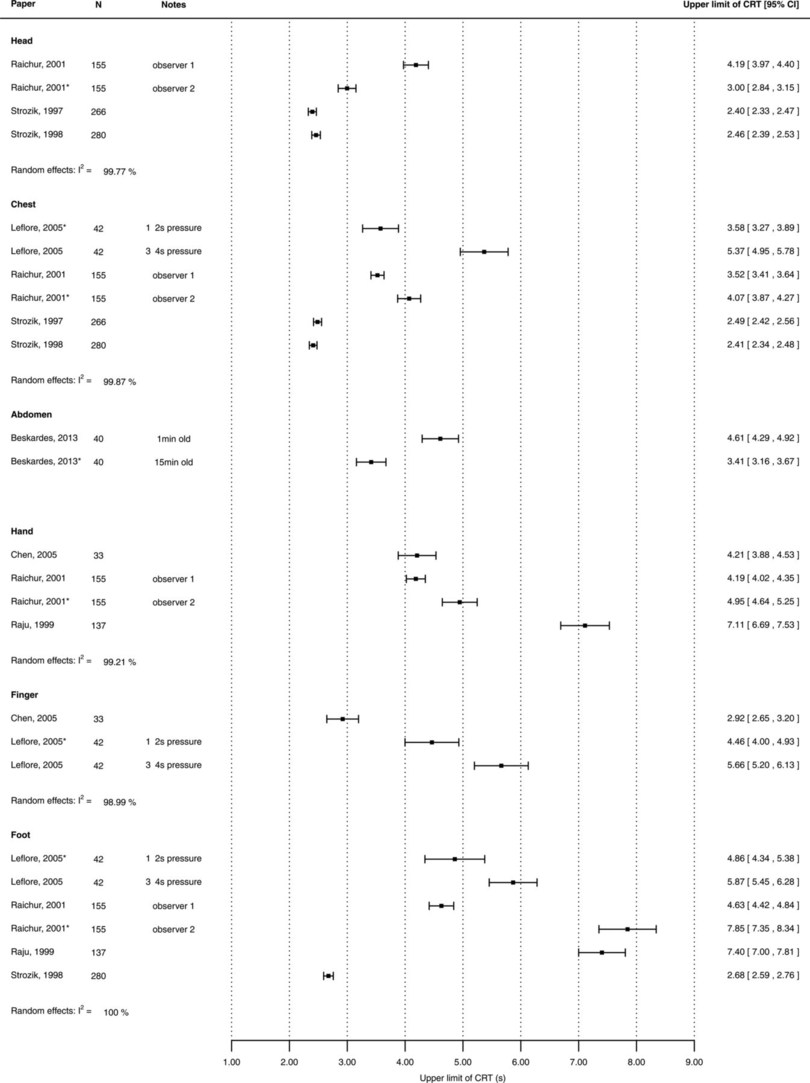
If you examine data from children older than 1 week, there is substantial heterogeneity, with capillary refill time on the chest being longer than is typically taught.
What we really want to know—the bottom line—is, ‘Is it any good?’ All healthcare providers perform the test daily on healthy and sick children, but is it warranted? It’s time to dive a little deeper.
Does the age of the child matter?
As we saw above, examiners assessing capillary refill time in neonates (at various anatomical sites, including the hands, feet, sternum, and forehead) found that the upper limit of normal was 3 seconds, not the 2 we usually use, and that it varied with age.
What about the temperature?
The few studies that have found no correlation between core temperature and CRT have found none. Making it of less value to detect a child with a fever.
However, the room temperature does make a difference. Gorelick et al. compared the CRT of healthy children of various ages in warm and cold rooms. When measured in the warm environment, they had a CRT of 0.85 ± 0.45 seconds compared to 2.39 ± 0.76 seconds. This meant that only 31% of those measured in the cold room would be considered to have a normal CRT. While this study is widely quoted, only 32 children were tested across a broad age range.
What’s the interobserver variability like?
If you use the kappa statistic from the Gorelick study, there appears to be only moderate interobserver reliability (κ = 0.54). This is not surprising, given that only 16 children were used to derive the value. Other studies have shown the kappa value to be as low as 0.14 – a near-worthless test if performed by different operators.
The kappa coefficient or statistic is a marker of interobserver reliability that considers that agreement could happen by chance. With a range of -1 to +1, a value of 0.14 indicates slight agreement and 0.54 moderate agreement. This, though, remains a matter of debate amongst querulous statisticians.
Champion, one of the proponents of CRT as a core sign in the assessment of shock in trauma, recommended against its use as it is difficult to assess in the dark. Delays in CRT are more difficult to detect under artificial light or in darker conditions.
So, how can we improve this? One way is to measure the refill time more accurately rather than counting out loud ‘One Mississippi, Two Mississippi’ and using a stopwatch. The same person should also repeatedly check the CRT rather than relying on a second observer.
So, how accurate is capillary refill time in sepsis or cardiovascular collapse?
Very little evidence of its value for such a widely used vital sign exists. Fleming’s review identified just four studies totalling 111 children. There is little correlation between CRT and blood pressure in neonates. PICU-based studies looking at CRT and central markers of poor cardiac outcome showed a positive predictive value of 93-96% and a negative predictive value of 40-50% to detect a ScVO2 of less than 70%.
A prolonged CRT ≥ 3 seconds is used as an ‘amber’ warning sign in the NICE traffic light guidelines, but these guidelines do not take into account the ambient temperature or anatomic location. A recent study published in Archives of Diseases in Childhood showed odds ratios crossing 1 for both pCRT and cCRT in the detection of serious bacterial infection.
What about CRT as a marker for dehydration?
Most of us have been taught that a prolonged CRT indicates possible dehydration. This assumption comes from data from Saavedra and colleagues, who even quantified it.
They suggested that a CRT of less than 1.5 seconds indicated a fluid deficit of less than 50ml/kg, a CRT of 1.5 to 3 seconds indicated a fluid deficit between 50 and 100ml/kg, and if the CRT was longer than 3 seconds, then there was a marked deficit of over 100mls/kg.
One must be aware that their average normal CRT was only 0.81 seconds (measured at the nail bed) and involved only 32 test subjects.
Capillary refill time varies with the child’s age, the anatomical site of testing, and the amount of pressure applied.
It is also impacted by ambient temperature and skin temperature.
If it is to be used, it should be done in a standardized way, using the same operator for repeat testing to eliminate inter-observer variability.
Trends are of more value than one-off measurements.
If you want more practice recognizing unwell infants, consider registering with www.spottingthesickchild.com.
What is the future of capillary refill time as a vital sign?
In the days of ECMO and REBOA, surely we should be better able to assess capillary refill time than just pressing on some skin and counting out loud? Perhaps there is some app we could use? (Editors note – please feel free to tell me there is)
High-speed digital photography has been used in experimental settings to determine the capillary refill rate in children with gastroenteritis accurately. However, the setting was a small single-centre trial, and the trial had its flaws.
Perhaps the boffins at MIT have the answer with Eulerian video magnification. If you don’t know what I am talking about, look at this brief video demonstration. The most minute changes in state can be identified by analysing imperceptible (to the naked eye) movements in individual pixels of a video image and then running them through a fancy algorithm. This might be the way of the future and a move toward wireless, non-contact, real-time assessment of vital signs.
The use of CRT to measure dehydration or cardiovascular collapse leaves much to be desired and is ripe for further study. Perhaps if we each performed a standardized measure on each child who comes through the ED with a minor injury or illness, we would have a better idea of normal in no time.
Acknowledgements
This post could not have been written without the help of the #ADC_JC from October 2014, helmed by Alan Grayson.
References
Beecher HK, Simeone FA, Burnett CH. The internal state of the severely wounded man on entry to the most forward hospital. Surgery 1947;22:672–81
Brown LH, Prasad NH, Whitley TW. Adverse lighting condition effects on the assessment of capillary refill. The American Journal of Emergency Medicine. 1994 Jan 31;12(1):46-7.
Crook J, Taylor RM. The agreement of fingertip and sternum capillary refill time in children. Archives of Disease in Childhood. 2013 Feb 9:archdischild-2012.
de Vos-Kerkhof E, Krecinic T, Vergouwe Y, Moll HA, Nijman RG, Oostenbrink R. Comparison of peripheral and central capillary refill time in febrile children presenting to a paediatric emergency department and its utility in identifying children with serious bacterial infection. Archives of Disease in Childhood. 2016 Jun 23
Fleming S, Gill P, Jones C, Taylor JA, Van den Bruel A, Heneghan C, Thompson M. Validity and reliability of measurement of capillary refill time in children: a systematic review. Archives of Disease in Childhood. 2015 Mar 1;100(3):239-49.
Gorelick MH, Shaw KN, Baker MD. Effect of ambient temperature on capillary refill in healthy children. Pediatrics. 1993 Nov 1;92(5):699-702. full text
Gorelick MH, Shaw KN, Murphy KO, Baker MD. Effect of fever on capillary refill time. Pediatric Emergency Care. 1997 Oct 1;13(5):305-7.
Lobos AT, Menon K. A multidisciplinary survey on capillary refill time: inconsistent performance and interpretation of a common clinical test. Pediatr Crit Care Med 2008;9:386-91
Raimer PL, Han YY, Weber MS, Annich GM, Custer JR. A normal capillary refill time of≤ 2 seconds is associated with superior vena cava oxygen saturations of≥ 70%. The Journal of Pediatrics. 2011 Jun 30;158(6):968-72. full text
Raju NV, Maisels MJ, Kring E, Schwarz-Warner L. Capillary refill time in the hands and feet of normal newborn infants. Clinical Pediatrics. 1999 Apr 1;38(3):139-44.
Saavedra JM, Harris GD, Li S, Finberg L. Capillary refilling (skin turgor) in the assessment of dehydration. Am J Dis Child 1991;145:296-8.
Schriger DL, Baraff L. Defining normal capillary refill: variation with age, sex, and temperature. Ann Emerg Med 1988;17:932-5.
Strozik KS, Pieper CH, Roller J. Capillary refill time in newborn babies; normal values. Archive of Disease in Childhood. 1997; 76:F193-F196.
Tibby SM, Hatherill M, Murdoch IA. Capillary refill and core–peripheral temperature gap as indicators of haemodynamic status in paediatric intensive care patients. Archives of Disease in Childhood. 1999 Feb 1;80(2):163-6.
“Really appreciated the detailed breakdown of capillary refill time! It’s amazing how such a quick and simple test can reveal so much about a patient’s circulatory and overall health. Understanding these subtle signs can make a huge difference in diagnosis. Thanks for explaining it so clearly and making this concept more accessible!