

| Topic | Common rashes |
| Author | Aoife Fox |
| Duration | Up to 2 hours |
| Equipment required | None |
- Basics (10 mins)
- Main session: (2 x 15 minute) case discussions covering the key points and evidence
- Advanced session: (2 x 20 minutes) case discussions covering grey areas, diagnostic dilemmas; advanced management and escalation
- Game
Quiz (10 mins) - Infographic sharing (5 mins): 5 take home learning points
We also recommend printing/sharing a copy of your local guideline.
Take a look at our Skin Deep project
BMJ Best Practice – Evaluation of rash in children
PEDS Cases – Viral Rashes in Children
Definitions/rash description:
- Macule: a flat area of colour change <1 cm in size (e.g., viral exanthem [such as measles and rubella], morbilliform drug eruption).
- Patch: a large macule >1 cm in size (e.g., viral exanthem [such as measles and rubella], morbilliform drug eruption).
- Papule: a raised area <1 cm in size (e.g., wart).
- Nodule: a larger papule, >1 cm in size (e.g. nodular prurigo).

- Plaque: a flat-topped raised area (a cross between a nodule and a patch; e.g., psoriasis).

- Vesicle: a small fluid-filled lesion (blister) <0.5 cm in size (e.g. varicella, eczema herpeticum).
- Bulla: a larger vesicle >0.5 cm (e.g. bullous impetigo).
- Pustule: a pus-filled lesion (e.g. folliculitis).
- Wheal: a transient raised papule or plaque caused by dermal oedema (e.g. urticaria)

- Scale: flakes of stratum corneum (e.g. eczema, psoriasis).
- Crust: dried serum, blood, or purulent exudate on the skin surface (e.g. impetigo).
- Erosion: loss of epidermis, heals without scarring (e.g. Stevens-Johnson syndrome, toxic epidermal necrolysis).
- Ulcer: loss of epidermis and dermis, heals with scarring (e.g. venous ulcer, pyoderma gangrenosum).
- Excoriation: loss of epidermis following trauma such as scratching (e.g. pruritus).

- Fissure: a split in the skin (e.g. angular cheilitis, palmoplantar keratoderma).
- Lichenification: thickening of the skin with accentuation of skin markings (e.g. chronic eczema, lichen simplex chronicus).

- Purpura: an area of colour change (red or purple) due to bleeding into the skin; does not blanch on pressure (e.g. vasculitis, disseminated intravascular coagulation).
- Petechia: a pin-point purpuric lesion (e.g.,vasculitis, disseminated intravascular coagulation).

- Ecchymosis: a larger area of purpura (e.g. vasculitis, disseminated intravascular coagulation).
- Where did the rash start?
- Sequence of the rash?
- Type of rash?
- Time of onset and duration?
- Involvement of palms and soles?
- Involvement of mucous membranes?
- Involvement of conjunctiva?
- Desquamating?
- Systemic involvement?
- Associated symptoms – fever/cough/conjunctivitis/runny nose/sore throat/strawberry tongue/itchiness/pain/weakness/headache/lymphadenopathy/swollen extremities/nausea/vomiting/diarrhoea?
- Exposures – immunizations/pets/foreign travel/bites (insects/ticks)/recent injury to skin/sexual history/sick contacts?
Common childhood rashes
The terminology for all but fifth disease is not used anymore, however, should anyone be curious here they are:
Forchheimer spots: rose coloured spots on the soft palate that may coalesce into a red blush and extend over the fauces
Koplik spots: clustered white lesions on the buccal mucosa. They are pathognomonic for measles.
Pastia lines: where pink or red lines formed of confluent petechiae are found in the skin creases.
Nagayama spots: erythematous papules on the mucosa of the soft palate and the base of the uvula. You may see these present on the fourth day in two thirds of patients with roseola.
(based on case from RCEM Learning RCEM Learning – Common Childhood Exanthems)
Mark is a 3-year-old boy brought to the ED by his mother with a rash, temperatures and decreased oral intake. His older brother has a similar rash and illness and mum reports that there was an outbreak of chickenpox in the older brother’s school.
On exam you note a quiet child with a diffuse vesicular rash. On palpation he has generalised lymphadenopathy.
What are the differentials of chicken pox in this case?
What is the incubation period of chicken pox? How long will Mark be infective?
What investigations are necessary?
How would you manage this illness? What treatment would you give?
What patients would you give anti-VZV immunoglobulin to?
Mark’s mum tell you that she has a 2-week old baby at home – what will you do?
What complications of chickenpox can occur?
Mum tells you that the children’s childminder is pregnant what advice do you give?
Discussion point – Do you use NSAIDs?
What are the differentials?
(Diffuse) disseminated gonococcaemia
(Local) hand, foot and mouth (coxsackievirus)
(Local) herpes zoster
Staphylococcal bacteraemia
What is the incubation period? How long will Mark be infective?
DFTB – Exclusion period for infections
The incubation period for chicken pox is usually 10-21 days. The infectivity period starts when symptoms first appear and lasts until all the lesions have crusted over. This is usually around 5-6 days after the onset of the illness, with most crusts disappearing by 20 days.
What investigations are necessary?
Chicken pox is a very common illness and the vast majority of cases can be managed symptomatically at home. Prolonged fever >4 days should prompt the suspicion of complications of varicella such as secondary bacterial sepsis. Under these circumstances, patients should be examined carefully with appropriate blood test work up and a chest x-ray, depending on their clinical presentation.
How would you manage this illness? What treatment would you give?
Oral acyclovir has been shown to reduce the effects of chicken pox, for example the number of lesions and duration of fever, if used within 24 hours of the onset of rash in immunocompetent children. Oral acyclovir has not been shown to reduce the incidence of varicella zoster virus pneumonia or other complications when compared to placebo. Cochrane results do not support the widespread use of acyclovir in immunocompetent children.
What patients would you give anti-VZV immunoglobulin to?
Pediatric EM Morsels – Chicken Pox
It is used for high risk patients including, immunocompromised children, newborns with maternal Varicella that develops 5 days before to 2 days after delivery, premature babies and hospitalized infants.
Mark’s mum tell you that she has a 2-week old baby at home – what will you do?
Paediatrics Open – Management of varicella in neonates and infants
Asymptomatic newborn in contact with VZV from any infected subject
The mother is proved seropositive:
Very low risk of disease in the baby.
No treatment should be provided.
Observance of the baby at home and encourage parents to come back if any clinical sign or symptom appears in the 2 weeks after contact.
The mother is proved seronegative or refuses testing:
Treat the baby with acyclovir PO 80 mg/kg/day divided into four doses to start 7 days after infective contact and administer during 7 days.
Careful surveillance of the baby during the risk period. Indication and duration of hospitalisation (with airborne and contact precautions) should be discussed in each case depending on child clinical status, parental compliance and social setting. If any doubt, hospitalisation with optimal medical surveillance are warranted during the risk period.
What complications of chickenpox can occur?
Pneumonia
Bacteraemia
Encephalitis
Bacterial superinfection of skin
Problems may arise where there is a failure to recognise the complications of secondary streptococcal or staphylococcal infections or to appropriately manage high-risk groups. A prolonged fever for more than 4 days in a child with chicken pox, for example, should prompt the suspicion of secondary bacterial complications.
A range of complications including pneumonia, bacteraemia and encephalitis are increasingly being recognised. Neurological complications may occur without a preceding rash.
The incidence of congenital varicella syndrome is low if maternal infection occurs before 20 weeks of gestation. Congenital varicella syndrome is associated with shortened limbs, skin scarring, cataracts and growth retardation.
Mum tells you that the children’s childminder is pregnant what advice do you give?
RCOG – Chickenpox in Pregnancy
The childminder should contact her own GP. She should avoid contact with children until establishing her risk of contracting VZV.
Do you use NSAIDS?
There is a long history of anecdotal evidence associating invasive group A Strep (GAS) complications, or severe skin and soft tissue infections (SSTIs) with exposure to NSAIDs.
There are currently 5 papers, ranging from 1997 to 2008 which try to answer this question. Almost all the studies used a case-control method to try and answer this question. Where they took a group of children who had varicella and the outcome of interest (invasive GAS infection, severe SSTI), and compared them to a group of children who had varicella and did not get these outcomes, seeing which groups were more likely to have had ibuprofen.
The studies are pretty heterogeneous, so unsurprisingly the results varied. These studies all found an association, but they generally all suffer from the same big problem, which is confounding by indication. It might not be that ibuprofen causes complications, but rather bad varicella needs ibuprofen, and is also more likely to get complications anyway. As the famous saying goes, “Correlation does not equal causation”. The absolute risk increase of GAS complications or SSTIs is 0.00016% in the worst case scenario.
NICE advises against giving ibuprofen due to the uncertainty but you must risk assess the clinical scenario yourself.
(Based on a case from the American Academy of dermatology – American Academy of Dermatology – Viral exanthems)
Caleb is a 9-year-old boy who presents for evaluation of fever and rash. His mother noted a fever of 40 °C two days ago. He appeared well and was eating and playing normally, so his mother was not alarmed. After the fever resolved, Caleb developed red rash that progressed rapidly over the past 24 hours.

What is the most likely diagnosis?
What are the differentials?
What is the cause of roseola?
Who gets it?
How is it spread?
What are the signs and symptoms of roseola?
How is it diagnosed?
What is the treatment?
What are the complications from roseola?
What is the most likely diagnosis?
Roseola
What are the differentials?
Measles
Rubella
Erythema infectiosum (fifth disease)
What is the cause of roseola?
It is caused most commonly by human herpesvirus 6 (HHV-6) and less commonly by human herpesvirus 7 (HHV-7).
Who gets it?
Children aged 6 months – 4 years are most typically affected. Most children (86%) will have had roseola by the age of 1 year. It is rarely seen in adults and infection is thought to confer lifelong immunity.
How is it spread?
It is spread person-to-person via the saliva of asymptomatic family members. The incubation period is 9-10 days.
What are the signs and symptoms of roseola?
It results in an acute febrile illness lasting between 3 and 7 days, which is then followed by the characteristic rash of roseola in around 20% of infected children.
The prodrome to the rash is a high fever (39-40 °C), palpebral oedema, cervical lymphadenopathy and mild upper respiratory symptoms. The child appears well. As the fever subsites the exanthem appear. This consists of a pink macules and papules surrounded by white halos. It begins on the trunk and spreads to the neck and proximal extremities. Nagayama spots may occur on the soft palate and uvula. The rash is non-itchy, painless and does not blister.
How is it diagnosed?
Diagnosis is usually based solely on the characteristic history and physical exam.
What is the treatment?
Roseola is usually benign and self-limiting. Rest, maintaining fluid intake and paracetamol for fever is all that is usually required. Treatment may be necessary for atypical cases with complications and immunosuppressed patients.
What are the complications from roseola?
Complications are rare in most children. The most common complication is febrile convulsion that occurs in 5-15% of children.
Acute encephalitis, hepatitis, myocarditis, haemophagocytic syndrome and infectious mononucleosis-like illness occur very rarely.
Reactivation of HHV-6 with drug exposure can lead to drug-induced hypersensitivity syndrome, which results in fever, rash, pneumonia, hepatitis, bone marrow suppression and encephalitis.
What advice would you give Caleb’s mother with regards to febrile convulsions?
Simple Febrile Convulsions generally occur in children aged from 6 months to 5 years. They are common affecting 1 in every 20 children. The most common causes are viral URTIs, ear infections, bacterial tonsillitis and UTIs.
They are generalised seizures, which last less than 15 minutes and occur only once during 24 hours.
The recurrence risk depends on child’s age at presentation: 1 year old: 50% recurrence;
2 year old: 30% recurrence
Where there are no neurodevelopmental problems and no family history of epilepsy, the subsequent risk of epilepsy is 1% (equivalent to the population risk).
A 5-year-old girl, Emma, attends the ED with after being unwell for the last 3 days. It initially started out with fever, headache and a sore throat. She then developed a rash 24 hours ago. Her parents report that the rash started on her abdomen and spread to the neck and arms and legs and it feels rough to touch.
On exam she has a sandpaper type rash on her trunk and limbs which is more pronounced in flexures.
What is the most likely diagnosis?
What other symptoms might Emma have?
What is it caused by?
What are the differential diagnoses?
How is the diagnosis confirmed? What investigations will you do?
What is the treatment? Why do you treat?
Discussion point – Evidence for antibiotic therapy
What are the possible complications? How can you categorise them?
What advice do you give to Emma’s parents in order to prevent transmission of Scarlet fever?
Is there anything else you need to do?
What is the most likely diagnosis?
Scarlet fever
What other symptoms might Emma have?
The symptoms of Scarlet fever start with fever (over 38.3°C), sore throat and general fatigue/headache/nausea. 12-48 hours later a rash appears on the abdomen and spreads to neck and extremities.
Characteristic features of the rash are a rough texture (like sandpaper) and worse in the skin folds e.g. groin, axilla, neck folds (Pastia’s lines).
Other symptoms include white coating on tongue which then peels and leaves a ‘strawberry tongue’; flushed red face with perioral pallor and cervical lymphadenopathy. Most symptoms resolve within a week. After the symptoms have resolved it is common to get peeling on the fingers and toes.
In Emma’s case the other symptoms that you would look for are – cervical lymphadenopathy, white tongue or strawberry tongue and a flushed face with peri-oral pallor.
What is it caused by?
Scarlet fever is caused by the bacterium Streptococcus pyogenes (also known as group A streptococcus, or GAS). It can be found on the skin or in the throat, where it is usually unproblematic in asymptomatic carriers – 20% of children are colonized.
However, certain virulent forms of S. pyogenes carry genes that code for streptococcal superantigens, including pyrogenic exotoxins, which can cause non-invasive infections such as scarlet fever. The typical rash is caused by the exotoxin.
What are the differential diagnoses?
They include measles, glandular fever, slapped cheek infections, other viral pathogens, Kawasaki disease, staphylococcal toxic shock syndrome, and allergic reactions.
How is the diagnosis confirmed? What investigations will you do?
The diagnosis is clinical. A throat swab is not routinely recommended, although during specific outbreaks Public Health England might advise this.
Streptococcal antibody tests are used to confirm previous group A streptococcal infection. They may be of value in patients with suspected acute renal failure, acute glomerulonephritis or rheumatic fever.
Antistreptolysin O (ASO) test is the most commonly available streptococcal antibody test. ASO titres peaks 2-4 weeks after an acute infection and returns to normal over the next 6-12 months. Streptolysin O is produced by almost all strains of S. pyogenes (group A streptococci) and many group C and group G beta-haemolytic streptococci.
Anti-deoxyribonuclease B (anti-DNase B (ADB)) titres rise after both pharyngeal and skin infections. DNase B is produced by group A streptococci and is therefore more specific than the ASO antibody test.
What is the treatment? Why do you treat?
General guidance for patients may include advice on rest, drinking plenty of fluids, good hygiene measures to minimise the risk of cross-infection, and the use of paracetamol to reduce discomfort and high temperature.
Overall, the evidence base for the management of scarlet fever is limited, and there is a need for more evidence of the benefits and harms of antibiotics.
Public Health England, NICE and the Department of Health in Western Australia recommend treating people with scarlet fever with antibiotics regardless of severity of illness to speed recovery, to reduce the length of time the infection is contagious, and to reduce the risk of complications.
Recommended antibiotic therapy is Penicillin V QDS x 10/7 or azithromycin OD x 5/7 if penicillin allergic.
What are the possible complications? How can you categorise them?
Complications of Scarlet Fever are much the same as complications of strep tonsillitis. They are divided into suppurative, and nonsuppurative.
Suppurative complications occur due to the infection spreading and include otitis media; mastoiditis; sinusitis; peritonsillar abscess; meningitis; endocarditis; retropharyngeal abscess; and invasive group A strep (IGAS).
Non-suppurative complications occur later and occur mainly in untreated patients. They are rheumatic fever and post-strep glomerulonephritis.
IGAS is not common in children, but those at increased risk are children with co-morbidities, immunocompromised children, and those with co-existing chickenpox.
What advice do you give to Emma’s parents in order to prevent transmission of scarlet fever?
(DFTB – Exclusion period for infections)
Children should be excluded from school until they have had 24 hours of antibiotics.
Is there anything else you need to do?
Check if you need to contact the public health authorities – scarlet fever is a notifiable disease in many jurisdictions e.g. England, Wales, Northern Ireland and Western Australia.

(Based on Life in the Fast Lane case – LITFL – Kawasaki Disease)
Alex, a 4 year-old boy has been brought to the emergency department by his worried parents. He has had fevers for the past 6 days. They are concerned because he is not getting better despite repeated visits to a number of doctors. Each time they were told he had a viral illness.
On examination you note the presence of bilateral conjunctivitis, and erythematous rash on his torso and limbs, a 4 cm tender left-sided cervical lymph node and a diffusely red pharynx.
What is the most likely diagnosis?
How is the diagnosis made?
Who gets this condition?
What are the important differential diagnosis?
What investigations should be performed?
What complications may occur?
What specific treatment is required?
Discussion point – Incomplete Kawasaki Disease: Another child, Sarah, attends the ED with 6 days of fever. On exam you find a strawberry tongue and cervical lymphadenopathy >1.5cm. No other signs of Kawasaki disease are present. What might you consider?
Discussion point – Is there a roll for steroids in Kawasaki disease?
What is the most likely diagnosis?
Kawasaki disease, also known as Mucocutaneous Lymph Node Syndrome, this vasculitic disorder was first described by Dr. Tomisaku Kawaski in 1967. It is of uncertain etiology, but may be a post-infectious condition.
How is the diagnosis made?
The diagnosis is made on the basis of the following clinical criteria (A + B):
| A. | Fever ≥5 days | |
| B. | At least 4 of the 5 following physical examination findings: |
| 1. | Bilateral, nonexudative bulbar conjunctival injectionbilateral scleral injection with peri-limbic sparing | |
| 2. | Oropharyngeal mucous membrane changespharyngeal erythema, red/cracked lips, and a strawberry tongue | |
| 3. | Cervical lymphadenopathywith at least one node >1.5 cm in diameter | |
| 4. | Peripheral extremity changesacute phase: diffuse erythema and swelling of the hands and feetconvalescent phase: periungual desquamation (weeks 2 to 3)The diffuse palmar erythema seen in KD is in contrast to the discrete macular lesions of various viral illnesses (e.g., measles) that can sometimes be seen on the palms and soles. | |
| 5. | A polymorphous generalized rashNon-vesicular and non-bullousThere is no specific rash that is pathognomonic for KD |
The manifestations may appear sequentially rather than concurrently. Atypical cases may not meet all the criteria but may still have the same risks of cardiac complications. These
‘incomplete’ cases occur more often in infants less than 6 months-old — further investigations (see Q5) should be performed if fever of 5 days and 2 or 3 of the other criteria are present.
Who gets this condition?
Kawasaki disease may occur in any child of any age, and even adults in some cases. However, it is more common in:
- children aged < 5 years
- child of Asian descent
- males (RR 1.5)
What are the important differential diagnosis?
Diagnosis may be difficult as Kawasaki disease may mimic a number of other conditions:
- Viral exanthemas including measles
- Streptococcal disease (e.g. scarlet fever, toxic shock syndrome)
- Staphylococcal disease (e.g. scalded skin syndrome, toxic shock syndrome)
- Bilateral cervical lymphadenitis
- Leptospirosis and rickettsial diseases
- Stevens-Johnson syndrome and Toxic Epidermal Necrolysis
- Drug reactions including mercury hypersensitivity reaction
- Juvenile Chronic Arthritis
What investigations should be performed?
Echocardiography —
this is the most important investigation to assess for cardiac complications.
If no abnormalities on presentation the study should be repeated in 4-6 weeks.
Laboratory tests
Rule out other causes:
— ASOT, AntiDNAse B, throat swabs, blood cultures
Non-specific findings seen in Kawasaki disease include:
— FBC: normochromic anaemia and leucocytosis; thrombocytosis (in the 2nd week)
— LFT changes and hypoalbuminemia
— increased CRP and ESR
— Sterile pyuria of ≥10 WBCs per high-power field
What complications may occur?
Cardiac complications:
- Carditis during the febrile phase
— myocarditis with ST-T changes (25%), pericardial effusions (20-40%), valvular dysfunction (1-2%) and cardiac failure (~5%) - Coronary vessel abnormalities (occur in 20% of cases if untreated and <5% if treated; peaks at 2-4 weeks)
— aneurysm formation may lead to fatalities from thrombosis, rupture or ischemia-related dysrhythmia (usually within 6 weeks of onset, but may occur many years later.
Kawasaki disease is a vasculitis that can potentially affect almost any organ, it is commonly associated with:
- arthritis
- keratitis and uveitis
- diarrhoea, vomiting and gallbladder disease
- coryza and cough
What specific treatment is required?
IV immunoglobulin and aspirin
IV immunoglobulin
- 2g/kg IV over 10 hours
- ideally start within 10 days of the onset of the illness
- a second dose may be given if fevers persist
Aspirin
- 3-5 mg/kg PO daily for 6-8 weeks
(when laboratory parameters have fully normalised) - some advise higher doses of aspirin until the patient is afebrile or 48-72 hours, but others argue this offers no benefit in addition to treatment with IV immunoglobulin.
Despite these therapies 2-4% of cases still go on to develop coronary artery abnormalities. Corticosteroids may be considered in refractory cases, although there is little evidence supporting their use.
Another child, Sarah, attends the ED with 6 days of fever. On exam you find a strawberry tongue and cervical lymphadenopathy >1.5cm. No other signs of Kawasaki disease are present. What might you consider?
Incomplete Kawasaki disease
Very easily missed
Makes up 15-20% of all cases
Patients with incomplete KD, particularly those <6 months of age and older children, may experience significant delays in diagnosis and these children are at high risk of developing coronary artery abnormalities.
Consider KD if:
- Infants <6 months old with prolonged fever and irritability
- Infants with prolonged fever and unexplained aseptic meningitis
- Infants or children with prolonged fever and unexplained or culture-negative shock
- Infants or children with prolonged fever and cervical lymphadenitis unresponsive to antibiotic therapy
- Infants or children with prolonged fever and retropharyngeal oroparapharyngeal phlegmon unresponsive to antibiotic therapy
Some pitfalls…
Fever and pyuria in an infant or young child may be diagnosed as a urinary tract infection, with subsequent development of rash, red eyes, and red lips attributed to an antibiotic reaction. Irritability and a culture-negative pleocytosis of the cerebrospinal fluid in an infant with prolonged fever suggestive of aseptic meningitis (or if antibiotics have been given, partially treated meningitis) may cause a diagnosis of KD to be overlooked. Cervical lymphadenitis as the primary clinical manifestation can be misdiagnosed as having bacterial adenitis. Gastrointestinal symptoms are considered for surgical causes, other physical findings of KD can be overlooked.
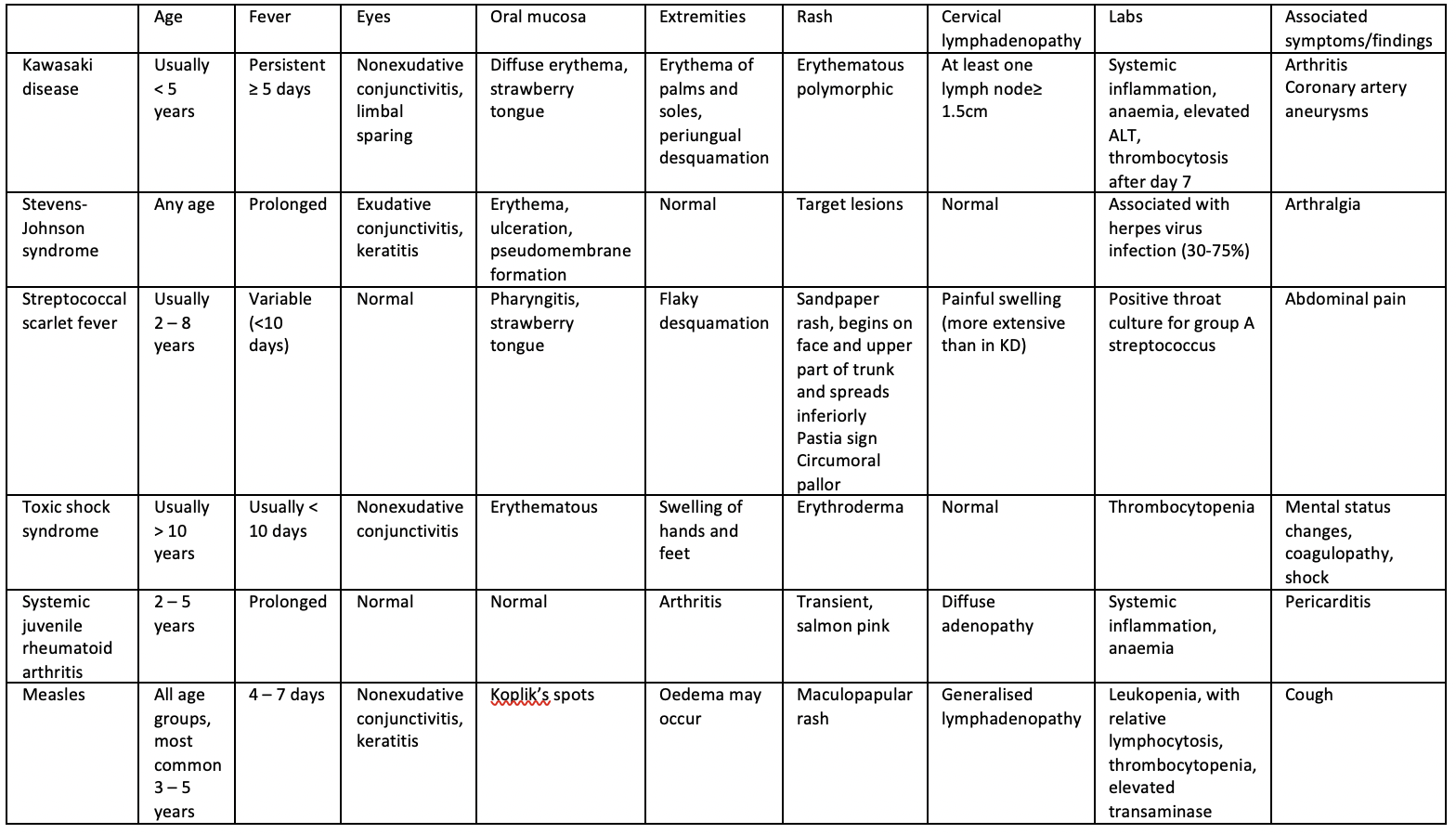
How could you differentiate between Kawasaki disease and scarlet fever?
Toxin-mediated illnesses, such as group A streptococcus infections (e.g. toxic shock syndrome and scarlet fever) can also present with fever, rash, mucous membrane involvement and abnormal extremity findings. Desquamation in Kawasaki disease tends to affect the hands and feet as it does in scarlet fever and toxic shock syndrome; however, in Kawasaki disease, it usually begins in the periungual region. In scarlet fever, the desquamation tends to be diffuse and flaking, whereas in Kawasaki disease it tends to be sheet-like.
How could you distinguish between incomplete Kawasaki disease and measles?
Children with measles and Kawasaki disease tend to be very irritable and inconsolable. It can be difficult securing the diagnosis of Kawasaki disease as the clinical features may appear sequentially rather than at the same time. In Kawasaki disease there may be presence of erythema and induration at the BCG immunisation site as there is cross reactivity between the heat-shock protein and the T-cells of patients with Kawasaki disease.
The temperature in measles may exceed 40°C but tends to fall after day 5 of the illness. Koplik spots are not seen in Kawasaki disease and the morbilliform rash of measles begins from the ears and hairline and starts to fade by day 4; after day 7 brownish staining may be seen due to capillary haemorrhage. Desquamation in severely affected cases of measles can occur but is not seen in the hands and feet. In measles, clinical improvement typically begins within 2 days of appearance of the rash.
This table can help distinguish between differentials:
Is there a role for steroids in Kawasaki disease?
(Cochrane – Using steroids to treat Kawasaki disease)
A Cochrane review published January 2017 concluded “steroids appear to reduce the risk of heart problems after Kawasaki disease without causing any important side effects. They also reduce the length of symptoms (fever and rash), length of hospital stay, and blood markers associated with being unwell. Certain groups, including those based in Asia, those with higher risk scores, and those receiving longer steroid treatment, may have greater benefit from steroid use, especially with decreasing rates of heart problems, but more tests are needed to answer these questions”.
Cards Against Paediatric Dermatology
https://em3.org.uk/foamed/9/8/2019/cards-against-paediatric-dermatology
Question 1
What disease is associated with dermatitis herpetiformis?
A: Herpes
C: Atopic dermatitis
D: Melanoma
Answer 1
The correct answer is B.
In coeliac disease, there are IgA antibodies against gluten that cross-react with reticulin fibres that anchor the basement membrane to the dermis. Thus, IgA is deposited at the tips of dermal papillae, presenting as grouped pruritic vesicles, papules or bullae. Usually found on elbows.
Question 2
What is the most common causative agent of erythema multiforme?
A: Penicillin and sulphonamides
B: Systemic lupus erythematosus
C: HSV infection
D: Malignancy
Answer 2
The correct answer is C.
HSV is the most common etiologic agent of EM, which presents as a targetoid rash and bullae. All the other options are also associated with the disorder, but less commonly.
Question 3
What disorder is characterised by an initial ‘herald patch’ which is then followed by scaly erythematous plaques usually in a ‘Christmas tree’ distribution?
A: Pityriasis rosea
B: Herpes
C: Varicella zoster virus
D: Erysipelas
Answer 3
The correct answer is A.
Pityriasis rosea classically presents with a salmon coloured solitary patch ‘herald patch’ which enlarges over a few days followed by generalised bilateral and symmetric macules with collarette scale. Pruritus is sometimes present. It itself resolves within 6 – 8 weeks.
Question 4
What is the infective agent implicated in acne?
A: Staphylococcus aureus
B: Streptococcus pyogenes
C: Staphylococcus epidermidis
D: Propionibacterium acnes
Answer 4
The correct answer is D.
Propionibacterium acnes infection produces lipases resulting in inflammation and breakdown of sebum, leading to pustule formation.
Question 5
Which of the following statements about the treatment of measles is correct?
A: No specific antiviral therapy is recommend for immunocompetent patients
B: Prevention of spread of measles depends on prompt immunization of people at risk of exposure or people already exposed who cannot provide documentation of measles immunity
C: Recommend supportive care with antipyretics, fluids and rest
D: All of the above
Answer 5
The correct answer is D.
BMJ Best Practice – Evaluation of rash in children
PEDS Cases – Viral Rashes in Children
RCEM Learning – Common Childhood Exanthems
DFTB – Exclusion period for infections
Pediatric EM Morsels – Chicken Pox
BMJ Paediatrics Open – Management of varicella in neonates and infants
RCOG – Chickenpox in Pregnancy
East Midlands Emergency Medicine Educational Media – Lightning Learning: Febrile Convulsion

The incidence of congenital varicella syndrome is low if maternal infection occurs before 20 weeks of gestation. Congenital varicella syndrome is associated with shortened limbs, skin scarring, cataracts and growth retardation.
I am just making a powerpoint on Dermatology and looking at chicken pox.
The link goes to CMV and in the light of the green book on advice with VZV I am not sure if this is accurate information:
It states:
“Why PEP is recommended for pregnant women
Chickenpox infection during the first 20 weeks of pregnancy can lead to fetal varicella syndrome, which includes microcephaly, cataracts, growth retardation limb hypoplasia, and skin scarring. Chickenpox can cause severe maternal disease and this risk is greatest in the second or early in the third trimester.
The rationale for PEP in pregnant women is two-fold: reduction in severity of maternal disease and theoretical reduction in the risk of fetal infection for women contracting varicella in the first 20 weeks of pregnancy. In late pregnancy, PEP may also reduce the risk of neonatal infection. However, given the risks of severe neonatal varicella in the first week of life, varicella zoster immunoglobulin (either as Varitect CP or IVIG) is also given to infants born within 7 days of onset of maternal varicella – (see section D3: infants and neonates).
Please can you kindly review this.
https://www.gov.uk/government/publications/post-exposure-prophylaxis-for-chickenpox-and-shingles/guidelines-on-post-exposure-prophylaxis-pep-for-varicella-or-shingles-january-2023#pregnant-contacts