

David is a 12-year-old boy who attends the emergency department complaining of bilateral heel pain. His pain has been getting gradually worse over the past month. He is a keen footballer, but his symptoms have gotten to the stage where he is now unable to play through his pain.
Apophysitis is a term used to describe a group of overuse traction injuries which commonly cause pain in adolescents.
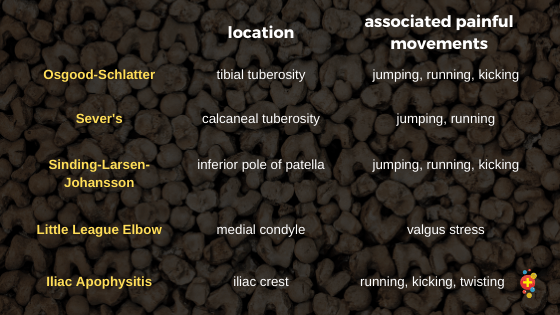
We have all heard of Osgood-Schlatter disease. It is the most common form of apophysitis. Other anatomical areas that are commonly affected include the inferior pole of patella (Sinding-Larsen-Johansson), calcaneal tuberosity (Sever’s), medial epicondyle of the elbow (within spectrum of Little League elbow) and various sites on the pelvis. They’re subtly different from osteochondrosis, which is instead due to changes in the epiphyseal ossification centre.
An apophysis is a bony growth separate from the ossification centres. It serves as a site of tendon or ligament attachment and eventually fuses with the bone as the body matures. Rapid growth and relative bone weakness, combined with repetitive movements, cause increased traction forces at the point of attachment. The apophysis is the weakest point in the muscle-tendon-bone junction; repeated strain at this point leads to bone fragmentation and micro-separation. This abnormal growth leads to swelling and pain at the site. Similar overuse injuries result in tendon and muscle injuries in adults.
Apophysitis is most common during the ages of peak growth, i.e. between 10-14 years in girls and 12-16 years in boys. Apophysitis is traditionally more common in boys, but the incidence is growing in girls. This is likely linked to increasing sports participation rates among girls of this age. The mean age of onset is lower in girls because the ossification centres appear earlier. Earlier fusion leads to the cessation of symptoms at a younger age in girls when compared to boys. In lower limb apophysitis, up to 50% of patients will experience bilateral symptoms.

{kind=link}

Let’s take a look at some X-rays
This 11-year-old male basketball player has been complaining of heel pain. His ankle x-ray shows increased density of the calcaneal apophysis, a finding typically seen in children aged 7 to 14 with Sever’s Disease. In addition, there is a loss of fat/soft tissue planes in the region of the retrocalcaneal bursa in keeping with acute inflammation.

This 12-year-old female long-distance runner complains of anterior knee pain, localised to the inferior aspect of her patella. Her lateral knee x-ray shows dystrophic ossification of the inferior patella with subtle thickening of proximal patellar tendon. These changes are consistent with a diagnosis of Sinding-Larsen-Johansson.

This 13-year-old female volleyball player presents with progressive pain over her tibial tuberosity. Her pain is exacerbated by jumping. Her lateral knee x-ray shows fragmentation of apophysis with overlying soft tissue swelling, classic for Osgood Schlatter Disease. Some isolated fragmentation can be normal at the tibial tuberosity.

This 11-year-old boy presents to the ED with worsening elbow pain. He is an avid cricket player and is trying to make his county underage team but finds his pain much worse while bowling. His AP elbow x-ray shows widening of the physis at the medial epicondyle. This is consistent with a diagnosis of Little League Elbow. You may also see fragmentation.

This is an MRI of a 14-year-old male long-distance runner complaining of anterior hip pain. His pain is becoming increasingly worse on running and is now affecting his times. MRI shows bone marrow and surrounding soft tissue oedema at the anterior superior iliac spine involving the sartorius muscle origin without separation as may occur in an acute avulsion injury. This is consistent with ASIS (anterior superior iliac spine) apophysitis. Plain radiographs are usually normal or may only show subtle changes of pelvic apophysitis.

History and exam
Apophysitis has a characteristic history, and the diagnosis is based primarily on a thorough history and exam. An adolescent will present with a gradual onset of focal pain over the involved site.
They are typically highly active and may be going through an acute increase in their training levels. They may currently be progressing to higher levels of sport or competing in multiple sports across multiple grades.
The initial symptom will be pain present at the start of physical activity. In the early stages, the pain often subsides once the child has fully warmed up, only to return when they cool down. As the process progresses, the child will have persisting symptoms throughout physical activity, and the pain will eventually result in total cessation of activity.
Clinical examination will reveal point tenderness over the affected site. There may be mild swelling over the area. Pain will be reproduced by resisted contraction of the affected muscle, e.g. resisted plantar flexion of the ankle in Sever’s disease and resisted knee extension in Osgood-Schlatter’s. A good way to assess this is to ask the patient to demonstrate actions which exacerbate their pain.
Differential diagnosis
Alternative diagnoses and investigations should be considered if there are any concerning features on history or exam. Atypical features on presentation are:
- Sudden onset of pain
- Pyrexia
- Non-weightbearing
- History of trauma
- Point of tenderness or age of patient not typical for apophysitis.
The most common differential diagnoses are osteomyelitis, avulsion fractures, osteochondritis, stress fractures and malignancy. Investigations should be performed in accordance with the suspected differential diagnosis.
The cases below and accompanying images highlight the need for you to have possible alternative diagnoses in the back of your mind. The patient should be presenting with gradual onset pain, over an apophysis site, at the appropriate age (10-16) for apophysitis. A history which includes high levels or a sudden increase in activity can be helpful. Any atypical features should be actively sought out.
This elbow x-ray is from a 13-year-old male baseball pitcher presenting with sudden-onset medial elbow pain. The medial epicondyle is displaced with a sliver of adjacent bone, representing a medial epicondyle avulsion fracture. There is marked adjacent soft tissue swelling and joint effusion. Compare this to the Little League elbow X-ray.

A 10-year-old female basketball player attended with sudden onset of knee pain following a fall. The x-ray shows a bone fragment avulsed from the inferior patella at the point of tendon insertion with moderate overlying soft tissue swelling: a patella sleeve fracture. This contrasts with the findings of dystrophic ossification of Sinding-Larsen-Johansson.

A 13-year-old female long jumper attends with anterior knee pain following a fall resulting in forced flexion of their flexed knee. She has significant pain and is unable to perform a straight leg raise. Her x-ray shows displacement of the tibial tuberosity with significant overlying soft tissue swelling: an avulsion fracture of the tibial tuberosity. Compare this to the typical radiographic features of fragmentation and mild swelling observed in Osgood-Schlatter disease.

A 13-year-old girl presents with worsening ankle/heel pain over the last week. Her pain is exacerbated on while running and playing football. She has been pyrexic over the past 24 hours and is now unable to weight bear. The x-ray of her ankle shows diffuse soft tissue swelling abutting the distal end of her fibula. There is suspicious erosion of distal fibular cortex. These findings are suspicious for osteomyelitis of the distal fibula.

An 8-year-old boy attends with gradual onset knee pain while running. He begins to notice some associated swelling. His mother feels he is becoming increasingly lethargic. Lateral x-ray shows sclerotic lesion involving the dia-metaphyseal region of the tibia with a wide zone of transition and characteristic “Sunburst ” type of periosteal reaction seen in osteosarcomas.

Investigations
Despite the diagnosis being clinical, a baseline x-ray is often useful. An x-ray can help ensure there is no avulsion fracture and a study by Rachel et al found x-rays changed management in up to 5% of patients with Sever’s disease.
Findings of apophysitis can vary on imaging and some patients may not show any radiological changes on plain films. The typical x-ray findings include increased density and fragmentation at secondary ossification centres. Overlying soft tissue swelling can often be seen. MRI will reveal increased fluid signal, apophyseal oedema and fragmentation.
This lateral plain film view shows the calcaneal apophysis with high density and fragmentation consistent with Sever’s disease.

Compare the x-ray to this MRI image showing oedema and fragmentation at the calcaneal apophysis and extending into the adjacent calcaneal tuberosity. These findings are commonly seen in patients with Sever’s disease.

Treatment
Apophysitis is a self-limiting process. Most patients will return to full activity following 4-6 weeks of rest or reduced activity. Despite successful return to activity, patients may continue to experience some symptoms. The symptoms will cease definitively once growth centres fuse.
The focus of treatment should be to reduce symptoms sufficiently to allow continued sports participation.
Strategies shown to improve recovery are
- analgesia
- activity modification
- muscle stretching and strengthening programmes
Other therapies which have little evidence but may be helpful in some cases, include
- ice application
- foot orthotics or heel raises in Sever’s disease
- taping or bracing
Surgery has no role in the standard treatment of apophysitis. Any short-term benefit observed from surgery cannot be justified when weighed against the potential damage to an immature skeleton. Surgery may be considered an option if there is a displaced avulsion fracture or a loose body in an affected joint.
Prevention
Apophysitis is largely preventable, and as a result, recent focus has been on primary and secondary prevention programmes. It can be difficult at the individual level to make changes, as these patients tend to be highly active and competitive. This has led some youth sport bodies to enforce limits on game participation and mandatory rest to avoid repetitive strain.
Simple advice to give parents and children includes:
- Encourage 1-2 days off from competitive sport per week
- Encourage 2-3 months off from each sport per year
- Participate on only one team per sport
- Avoid early sport specialisation
- Avoid increasing levels of training by more than 10% from one week to the next
- Maintain good sleep, hydration and dietary habits.
Take-home tips
- Apophysitis typically presents with gradual-onset pain over an apophysis in highly active adolescents.
- It is a self-limiting process, but it can cause debilitating pain.
- Treatment should focus on analgesia, activity modification, and muscle-stretching programmes.
- Symptoms will resolve definitively once ossification centres fuse.
Not to miss bits
Any atypical features should be investigated appropriately. The area around the apophysis is a common site for avulsion fractures, osteomyelitis and malignancy.
These patients are high risk for other overuse injuries. All patients should be given secondary prevention advice.
And our favourites, the controversies
- Despite the diagnosis being clinical, baseline X-rays can help rule out other differential diagnoses.
- There is little evidence displaying additional benefit for treatment with taping or splints.
- Custom orthotics can be useful for patients suffering from Sever’s Disease.
David undertook a month-long physio-led programme of activity modification and muscle stretching. He was given secondary prevention advice to avoid overtraining. He is now back to symptom-free football participation.
References
Brenner, J. S. (2007). Overuse Injuries, Overtraining, and Burnout in Child and Adolescent Athletes. Pediatrics, 119(6), 1242 LP – 1245
Elengard, T., Karlsson, J., & Silbernagel, K. G. (2010). Aspects of treatment for posterior heel pain in young athletes. Open Access Journal of Sports Medicine, 1, 223–232.
Fleisig, G. S., Andrews, J. R., Cutter, G. R., Weber, A., Loftice, J., McMichael, C., Hassell, N., & Lyman, S. (2011). Risk of serious injury for young baseball pitchers: a 10-year prospective study. The American Journal of Sports Medicine, 39(2), 253–257.
Frush, T. J., & Lindenfeld, T. N. (2009). Peri-epiphyseal and Overuse Injuries in Adolescent Athletes. Sports Health, 1(3), 201–211.
Gregory, B., & Nyland, J. (2013). Medial elbow injury in young throwing athletes. Muscles, Ligaments and Tendons Journal, 3(2), 91–100.
Guldhammer, C., Rathleff, M. S., Jensen, H. P., & Holden, S. (2019). Long-term Prognosis and Impact of Osgood-Schlatter Disease 4 Years After Diagnosis: A Retrospective Study. In Orthopaedic Journal of Sports Medicine (Vol. 7, Issue 10, p. 2325967119878136).
James, A. M., Williams, C. M., & Haines, T. P. (2013). “Effectiveness of interventions in reducing pain and maintaining physical activity in children and adolescents with calcaneal apophysitis (Sever’s disease): a systematic review.” Journal of Foot and Ankle Research, 6(1), 16.
Rachel, J. N., Williams, J. B., Sawyer, J. R., Warner, W. C., & Kelly, D. M. (2011). Is Radiographic Evaluation Necessary in Children With a Clinical Diagnosis of Calcaneal Apophysitis (Sever Disease)? Journal of Pediatric Orthopaedics, 31(5).
Ramponi, D. R., & Baker, C. (2019). Sever’s Disease (Calcaneal Apophysitis). Advanced Emergency Nursing Journal, 41(1), 10–14.
Vaishya, R., Azizi, A. T., Agarwal, A. K., & Vijay, V. (2016). Apophysitis of the Tibial Tuberosity (Osgood-Schlatter Disease): A Review. Cureus, 8(9), e780–e780.
Wiegerinck, J. I., Zwiers, R., Sierevelt, I. N., van Weert, H. C. P. M., van Dijk, C. N., & Struijs, P. A. A. (2016). Treatment of Calcaneal Apophysitis: Wait and See Versus Orthotic Device Versus Physical Therapy: A Pragmatic Therapeutic Randomized Clinical Trial. Journal of Pediatric Orthopaedics, 36(2).
Cairns G, Owen T, Kluzek S, et al. Therapeutic interventions in children and adolescents with patellar tendon related pain: a systematic review. BMJ Open Sport & Exercise Medicine 2018
Cairns, G., Owen, T., Kluzek, S., Thurley, N., Holden, S., Rathleff, M. S., & Dean, B. J. F. (2018). Therapeutic interventions in children and adolescents with patellar tendon related pain: a systematic review. BMJ Open Sport &Amp; Exercise Medicine, 4(1), e000383.