

Malcolm is nine years old. He jumped off the swing at the play park but tripped and fell onto his outstretched hands.
His left arm took the brunt, and he had severe pain and swelling in his left elbow after the injury.
He attends the local Emergency Department and is informed that he has a supracondylar fracture of his humerus.
Epidemiology of supracondylar fractures
Supracondylar fractures are common in children and account for about 60% of all paediatric elbow fractures.
The fracture occurs just above the elbow at the area of the distal humerus that is relatively narrow and weak in the immature skeleton. It is the most common fracture seen in children below the age of seven and the second commonest up to the age of 16.
95% result from a fall onto an outstretched hand with the elbow in full extension.
Presentation – History
Children usually present to the emergency department with a painful elbow they don’t want to move. They complain of swelling and bruising to the area. Because of the high incidence of neurovascular compromise with this fracture, they may also complain of loss of sensory or motor function in the affected hand.
Presentation – Examination
The examination can be difficult, especially when assessing the neurological status. Ensure adequate pain relief and a comforting environment whilst assessing the child.
Signs such as gross swelling, anterior bruising, skin puckering and deformity at the elbow indicate significant joint disruption.
This type of fracture has a particularly high complication rate. It is essential, as with all fractures, that the neurovascular status is thoroughly assessed and documented.
Finally, as with all injuries, we must thoroughly examine the joint below and above and assess for any other injuries on the child. The most common injury associated with a supracondylar fracture is the distal radius.
Investigations
Of course, we need an X-ray. The views required are an AP and true lateral of the elbow.
Most (97-99%) of these fractures are extension-type injuries. If there is displacement (25% have minimal or no displacement), it will most likely be posterior due to the extension mechanism. Only (1-3 %) are flexion-type injuries or are caused by a posterior blow to the arm resulting in anterior displacement.
To detect more subtle fractures, it is useful to have a strategy for assessing less obvious displacement. This can be achieved using the anterior humeral line (AHL). On a true lateral X-ray, a line drawn along the anterior surface of the humerus will intersect the middle third of the capitellum in most children >4 years old. In younger children, the AHL may lie in the anterior third of the capitellum.

The X-ray will also show abnormal fat pads unless the joint capsule is disrupted.

Make sure you look at the bigger picture. X-ray any other body parts where you suspect a fracture.
The Gartland classification
We can classify these fractures according to the degree of displacement: The Gartland Classification (see the image below):
- Type 1: minimal or no displacement of the fracture. There is a normal anterior humeral line on the X-ray. Often only abnormality is abnormal fat pads.
- Type 2: with posterior displacement, the posterior cortex remains intact and with anterior displacement, the anterior cortex remains intact.
- Type 3: completely displaced with complete cortical disruption.2
- Type 4: The periosteum is completely torn and is the most unstable type of fracture (can only be diagnosed intraoperatively).

Treatment: Immediate in the ED
Before examining or investigating, you must ensure the child has appropriate analgesia.
Keep the child nil by mouth as they may need urgent surgery.
Immobilise the elbow to 30-40 degrees in a long arm back slab to reduce pain, risk of compartment syndrome, neurovascular injury and loss of skin integrity (this can be done pre- or post-imaging depending on the amount of pain). It is important to monitor for any signs of these complications closely.
Treatment: Following imaging
Ongoing treatment depends on the degree of displacement.
Not displaced (Gartland type 1)
- Conservative management with either collar and cuff or long arm (above elbow) cast at 80-90° for 3 weeks (see areas of controversy below for more).
- Follow up in fracture clinic.
Displaced (Gartland type 2 – 4)
Above elbow cast at 30-40° to reduce the chance of neurovascular injury and manage pain.
These require surgery on the day of injury but not overnight unless neurovascular or skin compromise:3
- No radial pulse
- Signs of reduced perfusion to the hands
- Skin viability threatened
- Evidence of nerve injury
Many trusts will have local guidance from the orthopaedic team about specifics of management, referral and follow-up, so refer to your departmental policy.
If the fracture is open: manage the wound conservatively and administer antibiotics appropriately.
As with all paediatric situations: consider NAI if the injury appears more significant than the history would suggest, especially if under two years old.
Operative management
The British Society for Children’s Orthopaedic Surgery recommends bicortical wire fixation when operative management is required. This is with closed manipulation under anaesthesia. Open reduction increases the risk of infection and stiffness.
If the limb is perfused, but no radial pulse is present, it is not recommended that the brachial artery is explored. However, if the limb is ischaemic before theatre; the orthopaedic team must alert a vascular team expert in small vessel repair, as an exploration of the artery may be required if fracture reduction fails to re-perfuse the limb.
Most nerve injury caused by the fracture or operative management is transient neuropraxia and can be managed expectantly.
Areas of controversy
Traditionally displaced supracondylar fractures were reduced as an emergency, whether or not there was neurovascular injury. It has been shown that there are increased iatrogenic complications if the surgery is done overnight. It is recommended that only injuries with compartment syndrome, neurovascular injury or loss of skin integrity are operated on overnight.
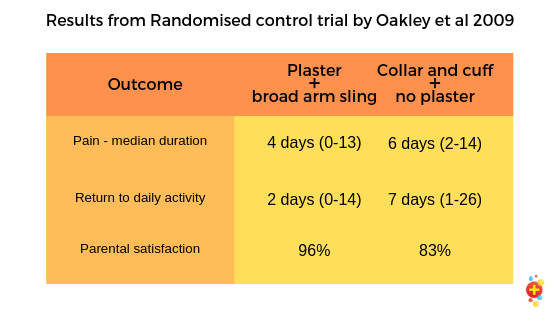
Gartland type 1 fracture should be managed conservatively with immobilisation. This could be by plaster or collar and cuff, with some centres preferring the collar and cuff method. A randomised controlled trial by Oakley et al. 2009 compared the use of above elbow plaster immobilisation to collar and cuff without plaster (n=50, 27 with plaster and 23 with collar and cuff). The outcomes assessed were pain, resumption of the child’s normal activities and parent satisfaction. None of the patients had fracture displacement or neurovascular compromise at the 2-week check, all had a degree of motion impairment, and there were similar immobilisation device issues between the groups. The table below describes the primary outcomes of the study.

{kind=link}
Potential complications
Vascular injury
- The brachial artery lies anterior to the humeral cortex at the supracondylar region, and therefore the fracture can impinge on the brachial artery causing significant vascular compromise.
Nerve injury
- 11% will have associated nerve injury, most commonly the anterior interosseous nerve – check the child can make the “OK” sign (flexion of thumb IPJ and index finger DIPJ).
- The less common flexion injuries can result in ulnar nerve damage – check finger abduction and sensation to the ulnar border of the little finger.
- The median nerve is at risk of injury though is structurally stronger and less likely to be injured than the brachial artery. Apparent nerve injury is usually transient.
- Look at our elbow examination post for a reminder of how to assess peripheral nerve function.
Compartment syndrome
- Bleeding from an injured vessel and swelling in the region can induce compartment syndrome and cause further neurovascular and muscular injury.
- The median nerve and radial artery can be compressed in the forearm’s anterior compartment.
- Remember: loss of radial pulse is a late sign of compartment syndrome!
Volkmanns Ischaemic contracture
- Prolonged reduction in blood supply to the muscles results in necrosis and later fibrous replacement of the muscle tissue. This can be due to delayed reperfusion of an ischaemic limb and/or compartment syndrome. This results in an irreversible flexion of the fingers and wrist and pronation of the wrist, which is disabling.
Malunion
- A good reduction position is required to reduce the risk of deformity.
Myositis ossificans
Bone growth in the muscle can occur in this type of fracture.
Things not to miss!
Take a good look at the X-ray: are the fat pads normal? Is the anterior humeral line normal?
Carefully check and DOCUMENT neurovascular status. Make sure this is closely monitored.
The anterior humeral line may not be reliable in very young children as the capitellum may only be partially ossified but normal. If in doubt: seek expert help.
Case resolution
Malcolm was found to have a weak radial pulse and was taken straight to theatre from the ED. He had an external manipulation and wire placement and an uncomplicated recovery. He had an X-ray in 5 days and was noted to have a satisfactory position. The wires and plaster were removed in 3 weeks, and he was back on the swing five days later…
Selected references
Raby N, Berman L, Morley S, de Lacey G. 2015. Accident and Emergency Radiology: A survival Guide Third Edition, Sauders Elsevier page 106-110.
British Orthopaedic Association Standards for Trauma (BOAST), British Society for Children’s Orthopaedic Surgery (2014) BOAST 11: SUPRACONDYLAR FRACTURES OF THE HUMERUS IN CHILDREN. Accessed 19/03/2019 <https://www.boa.ac.uk/resources/boasts/boast-11-pdf.html>
St. Clair BJ & Schreiber VM. Supracondylar Humerus Fractures. Operative Techniques in Orthopaedics. 2019 29:11–16. doi.org/10.1053/j.oto.2018.12.003
Saeed W, Waseem M. Elbow Fractures Overview. 2019 Jan 20. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from PubMed PMID: 28723005.
Herman MJ, Boardman MJ, Hoover JR & Chafetz RS. Relationship of the anterior humeral line to the capitellar ossific nucleus: Variability with age. Journal of Bone and Joint Surgery. 2009; 91(9):2188–2193
Dandy DJ, Edwards DJ, 2003. Essential Orthopaedics and Trauma, Fourth Edition, Churchill Livingstone page 193-5
American Academy of Orhopaedic Surgeons, 2014. Appropriate use criteria for the management of pediatric supracondylar humerus fractures. Accessed 19/03/2019 <>
Vaquero-Picado A, González-Morán G, Moraleda L. Management of supracondylar fractures of the humerus in children. EFORT Open Rev. 2018 Oct 1;3(10):526-540. doi: 10.1302/2058-5241.3.170049. eCollection 2018 Oct. PubMed PMID: 30662761; PubMed Central PMCID: PMC6335593.
Oakley E, Barnett P, Babl FE. Backslab versus non-backslab for immobilization of undisplaced supracondylar fractures: a randomized trial. Pediatr Emerg Care. 2009 Jul;25(7):452-6. doi: 10.1097/PEC.0b013e3181ab7898. PubMed PMID: 19564806
Davies FCW, Bruce CE and Taylor-Robinson K. Emergency are of minor trauma in children. 2011. London: Hodder & Stoughton
Hill CE and Cooke S. Common Paediatric Elbow Injuries. The Open Orthopaedics Journal. 2017; 11: 1380–1393
Hi Lisa Dunlop,
This supracondylar fracture post is really super. The way you described everything is really easy to understand. I really love this blog. I hope you will be doing well in trauma and toxicology as well.
Thanks.