

Little fingers get everywhere, and injuries are common. The mechanism of injury tends to be age-dependent, with the under-fives magnetically drawn to door hinges and the over-fives more likely to do some damage during higher-impact sports. Below are a few common injuries of the tendons and collateral ligaments of the fingers that you might come across in PED.
Ensure adequate analgesia before assessment. Occasionally, a local anaesthetic is required—don’t forget bubbles, too!As tendon/ligament injuries may not occur in isolation, an assessment must include inspection, palpation (look, feel, move!), assessment of vascular structures, and testing of motor and sensory functions.Children typically tend to display hand dominance between the ages of 2 and 4; if the child is old enough, make sure to record hand dominance in the medical or nursing notes.In older children/adolescents, document details of sports participation/ hobbies/professional goals as these may be considered by hand surgeons when considering treatment options.
Part 1: Flexor tendon injuries
Anatomy
There are two flexor tendons for each finger and one for the thumb.
The flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) are the flexor tendons of the fingers, and the flexor pollicis longus (FPL) is the only thumb flexor.
The flexor tendons travel distally from the forearm through the carpal tunnel and are named based on the forearm muscles from which they arise.
The flexor digitorum profundus (think profound, i.e. deep) arises from the deeper layer of the flexor muscles. The flexor pollicis longus tendon of the thumb also arises from the deeper muscle layer. The flexor digitorum superficialis (think superficial) continues the more superficial layer.
- FDP inserts at the base of the distal phalanx and flexes the DIP joint (tip: FDP is at the point of the finger).
- The FDS tendon divides into two slips that wrap around the FDP to insert into the sides of the middle phalanx. FDS flexes the PIP joint.
")
The Pulley System
The flexor tendons are enclosed in a synovial sheath that lubricates them and minimizes friction.
It is organized into segments of transverse fibres forming annular pulleys (annular means ring-like; think of the ring-like lesions of annular eczema) and oblique fibres comprising cruciate pulleys (cruciate means crossed, like the cruciate ligaments of the knees).
There are three cruciate pulleys (C1-3) and five annular pulleys (A1-5) pulleys. These pulleys keep the flexor tendons close to the bone and prevent bowstringing of the tendon.

Evaluation
Closed flexor tendon injuries are usually caused by forced extension of the finger in active flexion. The child may present with reduced finger flexion or pain when bending the finger, and there may be localized swelling or open wounds.
The FDS and FDP tendons should be tested individually; it is not enough to observe the child make a fist, as tendon injuries can be easily overlooked or missed.
To check FDS function, hold all adjacent fingers in extension and then release the finger you want to assess. Ask the child to flex the free digit at the PIP joint.
To examine the FDP, hold the middle phalanx in extension and ask the child to flex the DIP joint.


Examination Pearls
Tendon function can be difficult to assess in a young or uncooperative child. In these circumstances, observation of digital cascade and wrist tenodesis can be useful physical examination tools to assess tendon integrity of the hand and fingers.
Digital Cascade
When the child’s hand is in a resting position, the fingers should have a natural cascade of progressively increasing flexion from the index finger through to the little finger.

Wrist Tenodesis
Squeezing the forearm muscles while observing the fingers can also be used to assess flexor tendon continuity. If flexor tendons are intact, the child’s fingers should flex when the forearm muscles are squeezed.

A: Extending the wrist flexes the fingers. With intact flexor tendons and a relaxed or distracted patient, passive wrist extension results in finger flexion. If flexor tendons are damaged, the injured finger(s) will rest in an extended position when the wrist is extended.
B: Flexing the wrist extends the fingers. Similarly, with intact extensor tendons, passive wrist flexion results in finger extension. If the extensor tendons are damaged, the injured finger(s) will rest in a flexed position when the wrist is flexed.
Wound Exploration
It is important to remember that tendons move; looking into a wound and seeing an intact tendon does not exclude a tendon injury. If the wound is sustained while the finger is flexed and the finger is examined while it is extended, the level of the tendon injury will not correspond to the level of the skin laceration. Therefore, it is important to ask the parent or older child/adolescent about finger position at the time of the injury and put the injured digit through a passive range of movement while examining the wound. If you doubt or cannot rule out a tendon injury, refer the patient to the local hand surgery team.
Classification
The sites of the flexor tendon injuries are divided into five zones.


*The term ‘No Man’s Land’ was coined by hand surgeon Mr Sterling Bunnell in 1918 because, at that time, it was felt no man (or woman) should attempt repair within this zone due to the complexities of the anatomy and risk of adverse outcomes. While this belief is no longer a common practice, it highlights the intricacies of surgical repair within this zone.
Jersey finger (Zone 1 injury)
Juno is a fifteen-year-old girl attending ED with an injury to her left ring finger.
She was playing rugby earlier today, and her hand got caught in another player’s jersey during a tackle.
On examination, you note swelling, bruising, and tenderness to the volar base (on the palmar side) of her distal phalanx on her left ring finger. When you lie her left hand flat on a table with the palm facing upwards and hold the middle phalanx of her ring finger in extension, she cannot flex her distal phalanx at the DIP joint. She also can’t bend the DIP joint when trying to make a fist.
You correctly identified that she has an injury to her FDP tendon and diagnosed Jersey Finger. You send Juno to X-ray to assess for a fracture.

Mechanism
Disruption of the FDP tendon is known as Jersey finger. This injury is caused by the forced extension of the DIP joint during active flexion. It commonly occurs when an athlete’s finger catches in another player’s jersey, usually while playing a tackling sport such as rugby or American football. For those who prefer more solo pursuits, it can also be caused by an overly tight crimp grip in climbers.
Presentation
A patient with a Jersey finger may present with pain and swelling to the volar (the palmar) aspect of the DIP joint, and the finger will be extended at rest. The ring finger is commonly affected. The integrity of the FDP should be evaluated as outlined above. An injured FDP will produce very restricted or no movement. An x-ray should be performed to rule out an avulsion fracture at the volar base of the distal phalanx.



Treatment
Early referral to a hand surgeon for assessment and appropriate treatment is paramount.
Operative: The majority of these cases require surgical intervention to reattach the tendon, prevent tendon retraction, and optimize function. The prognosis for patients with Jersey finger worsens if treatment is delayed and severe tendon retraction is present.
Non-Operative: A partial tear may be managed conservatively (splinting, NSAIDs, physiotherapy). However, from a PED perspective, these injuries should be considered surgical cases until deemed otherwise by a hand specialist.
You do not identify a fracture on Juno’s X-ray, and you refer her to the Plastic Surgery team for prompt review, as she may require surgery to repair her FDP tendon.
…A quick overview of Trigger thumb
Trigger thumb, although uncommon, may be a reason for presentation to the PED, typically when a child is two years old. Paediatric Trigger thumb results from a mismatch in the size of the Flexor Pollicis Longus (FPL) and the first annular pulley (A1), disrupting normal tendon gliding. Children find it difficult to extend the IP joint of the thumb, with clicking or snapping felt or heard. Some patients even have a fixed flexion deformity at the IP joint. Characteristically, a palpable mass is felt at the level of the MCP joint crease on the thumb’s volar (palmar) surface, representing a nodule in the FPL and thickening of the flexor tendon sheath. This is commonly referred to as ‘Notta’s Node’.
Its aetiology is poorly understood. Historically, the trigger thumb was thought to be congenital. However, this is controversial, and an argument exists that trigger thumb is an acquired condition. Diagnosis is usually based on clinical exam. X-rays or alternate imaging are rarely indicated, although parents will occasionally try to attribute symptoms to a recent history of trauma. This is usually a red herring!
Paediatric trigger thumb can be managed surgically or conservatively with splinting and a physiotherapy regime. Sometimes, it can spontaneously resolve, although the spontaneous resolution of paediatric trigger thumb can be less likely after two years old. Surgical release of the first annular pulley may be offered as a treatment option to restore thumb IP joint movement if there is a fixed flexion deformity beyond 12 months of age or if conservative management fails.

Part 2: Extensor Tendon Injuries
Anatomy
Distal to the MCP joint, the common extensor tendon divides into three slips: one central and two lateral bands. The central slip inserts at the base of the middle phalanx, and the two lateral bands extend along the radial and ulnar margins of the middle phalanx to converge at the distal third of the middle phalanx to form the terminal extensor tendon, which inserts at the base of the distal phalanx. The central slip extends the middle phalanx at the PIP joint level, and the terminal extensor tendon extends the DIP joint. The Extensor Pollicis Longus (EPL) extends the thumb at the IP joint.

Evaluation
The extensor tendons are assessed by applying pressure to the dorsum (back) of the finger while the patient is attempting active extension.

To test the Extensor Pollicis Longus (EPL), ask the patient to place their hand flat on a table and lift up their thumb against resistance.

Classification
The extensor mechanism can be divided into nine anatomical zones. Odd-numbered zones are located over joints, and even-numbered zones are located over bones. Tendon injuries can be categorized according to these anatomical zones.

A little nugget: an easy way to recall the extensor zones is to remember the odd numbers (I, III, and V) are at the joints (DIPJ, PIPJ, and MCPJ).
Injuries in Zone 1 (the DIP joint) and Zone III (the PIP joint) cause unique injury patterns, which we’ll explore below.
The thumb has a unique classification system as it has one fewer phalanx.
Mallet Finger: zone I injury (Baseball Finger)
Isabelle is an 8-year-old girl who was playing with her twin sister, Sophie, in their bedroom while their Mummy and Daddy were busy working from home in another room. Sophie accidentally closed the bedroom door, catching Isabelle’s finger in the hinge side of the door.
In ED, you see that Isabelle’s right dominant index finger is bruised and swollen at the DIP joint, and there is a superficial abrasion to the dorsum of the DIP joint. Isabelle’s point of maximal tenderness is to the DIP joint. You try to assess finger function, but Isabelle cries and says she is too sore to move her fingers. But you note that the index finger appears flexed at the DIP joint, and you suspect a Mallet injury. You give Isabelle analgesia and refer her for an x-ray.
Mechanism
Mallet finger is a partial or complete avulsion of the terminal extensor tendon from its insertion on the distal phalanx, commonly resulting from sudden flexion of an extended DIP joint. It can also occur secondary to a crushing mechanism.
Presentation
Mallet finger can be an open or closed injury with or without a fracture. Patients present with a flexion deformity at the distal phalanx and an inability to extend the finger at the DIP joint, which can be swollen and ecchymosed.

In children, this injury typically occurs due to an avulsion fracture of the distal phalangeal epiphysis, the insertion point of the terminal extensor tendon.

Classification
Mallet fingers can be described using a classification scheme (I through IV) developed by Doyle (1993).

Treatment
Early referral to a hand surgeon for assessment and advice regarding appropriate treatment is essential.
Non-operative: Closed acute injuries with or without fractures can be managed with 6-8 weeks of extension splinting at the DIP joint, followed by gentle active flexion ROM.
A 2004 Cochrane review found insufficient evidence to support the use of any particular splint when treating mallet injuries; all achieved similar outcomes. However, patient compliance is vital to a successful outcome.
Operative: Open injuries are treated by surgical repair.
Closed injuries may be considered for surgical management if there is joint subluxation or an avulsion fracture of more than 30-50% of the articular surface.
Complications: Swan-neck deformity
Correct management of an acute mallet injury is critical, as a poorly managed or untreated chronic terminal extensor tendon injury can lead to swan-neck deformity.
The swan-neck deformity is caused by prolonged DIP flexion with dorsal subluxation of lateral bands and PIP joint hyperextension.

It takes a while before Isabelle and her Mum return to the ED for X-ray. Fortunately, the analgesia seems to have had some effect, and Isabelle is more relaxed. You reviewed the X-ray and did not identify a fracture.
On examination, you confirm a flexion deformity at the DIP joint and note that Isabelle cannot actively extend at the DIP joint. Suspecting a mallet injury, you apply an extension splint and refer Isabelle to plastics. They opt to treat the injury conservatively with an extension splint at the DIP joint for six weeks. They give Mum and Isabelle careful advice about compliance with splinting and give her an appointment for follow-up in outpatients.
Central Slip Injuries: zone III injury
Michael is a talented 15-year-old basketball player. Three days ago, he was playing in a school league basketball final when he felt a sudden sharp pain in his left middle finger after a failed attempt at catching the ball. He played until the end of the game but attended a minor injuries unit the following day, as his finger was swollen and painful at the PIP joint.
After a normal X-ray, he was diagnosed with a soft tissue injury and discharged home with his fingers buddy-strapped. However, his pain has not improved, and he can’t fully extend his finger at the PIP joint, so his dad brings him to your ED. He has a digital copy of the X-Ray for you to review.
Mechanism
Central slip injuries are extensor tendon injuries at the middle phalanx, often resulting from forced flexion of an extended PIP joint, a mechanism commonly seen in basketball players. Other injuries that can accompany central slip disruption include volar (palmar) dislocations of the PIP joint, dorsal avulsion fractures of the base of the middle phalanx, and lacerations to the dorsal surface of the PIP joint.
Presentation
The PIP joint may be swollen and bruised. The area of maximal tenderness is generally over the dorsal aspect of the PIP joint.
Closed central slip injuries can be easily missed or misdiagnosed as sprains or soft tissue injuries as there is no wound and sometimes no abnormality seen on X-ray.
The physical examination can be challenging. Some patients have no loss of active extension at the PIP joint, as extension is still provided by the lateral bands of the extensor tendon despite the disruption of the central slip. Even when there is a loss of extension, this can be overlooked or attributed to pain. (Don’t forget to provide adequate analgesia before assessment!)
These pitfalls can be avoided by maintaining a high index of suspicion for a central slip injury and undertaking a careful examination, including Elson’s test to establish the integrity of the central slip, especially in the patient who presents with a painful, swollen PIP joint without gross deformity. Occasionally, ring blocks are required to allow a proper assessment of ROM.
Elson’s Test
-
Ask the patient to bend the affected PIP joint 90° over the edge of a table and ask them to extend the middle phalanx against resistance.
-
If the central slip is intact (negative test), extension is strong, and the DIP remains floppy because the extension force is now placed entirely on maintaining extension of the PIP. The lateral bands cannot act distally in this position.
-
When a rupture of the central slip is present (positive test), there will be weak PIP extension, and the DIP will extend abnormally and become rigid.
A modified version of Elson’s test can also be used. Here’s how the Modified Elson’s Test is done:
-
Ask the patient to place their injured and uninjured contralateral fingers knuckle to knuckle in 90-degree PIP flexion, with the middle phalanges pressed against each other. The patient is then asked to extend both DIP joints.
-
Negative test (normal)- DIP joints symmetrically flexed.
-
A positive test (central slip injury)- Injured DIP joint extends more (See diagram below).

This video from Brian Lin demonstrates both tests beautifully.
These tests can be limited by pain and the patient’s ability to cooperate. If a closed central slip injury is suspected, then the PIP joint should be splinted in an extension and follow up in a hand clinic.
Treatment
Early referral to a hand surgeon for assessment and advice regarding appropriate treatment is essential.
Non Operative:
- Closed injuries
- Extension splinting of the PIP joint for up to 6 weeks to allow central slip restoration
Operative: Surgical treatment reserved for
- Open injuries
- Displaced avulsion fractures of the middle phalanx
- PIP instability
- Failed non-surgical treatment
Complications: Boutonnière deformity
Failure to recognize and treat a central slip injury in the ED may result in a problematic Boutonnière deformity later.
Boutonnière deformity is characterized by flexion of the PIP joint and hyperextension of the DIP joint. It develops secondary to loss of extension force on the PIP joint, with volar subluxation of the lateral bands and subsequent DIP joint hyperextension.

On examination, you note swelling and bruising to the PIP joint. Michael tells you that he is maximally tender on palpation to the dorsal surface of his PIP joint. He is able to partially extend his finger at the PIP joint but using Elson’s test, you note weak PIP extension and an abnormally extended and rigid DIP joint.
You diagnose a central slip injury and explain the diagnosis to Michael and his dad before referring Michael to the plastic surgery team for assessment. Plastics treat Michael in an extension splint for six weeks to allow central slip restoration.
Part 3: Collateral Ligament Injuries
Anatomy
The collateral ligaments stabilize the phalanges laterally at the DIP, PIP and MCP joints.

Mechanism
Forced ulnar or radial deviation of IP joints can cause partial or complete collateral ligament tears.
Presentation
Collateral ligament injuries of the fingers present as tenderness on palpation overlying the affected ligament, swelling, and sometimes bruising.
Evaluation
The integrity of a collateral ligament is assessed by applying valgus and varus stress to the involved joint with the joint in full extension and with the joint in 30 degrees of flexion. Compare the laxity of the injured finger with an unaffected finger. Increased laxity or lack of an endpoint signifies an injury.
An x-ray should be performed to out-rule an avulsion fracture at the insertion site of the ligament.
Treatment
If the joint is stable and no large fracture fragments are identified, the injury can be treated with buddy strapping.
Treatment Pearl: Buddy strapping
If the ring finger is involved, it should be secured to the little finger as it is naturally extended and easily injured if exposed.
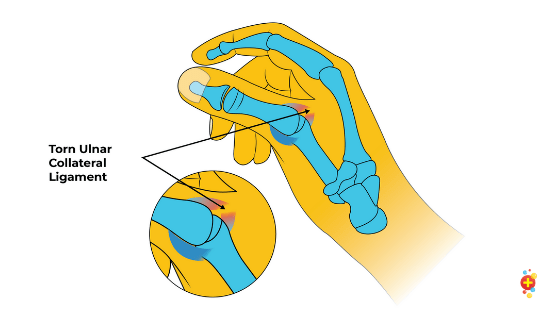
Ulnar Collateral Ligament Injury of the Thumb (Skier’s Thumb / Gamekeeper’s Thumb)
Tess was excited as she stepped out onto the fresh, crunchy snow, all kitted up and raring to go. However, she didn’t count on it being so slippery and fell more or less right away whilst holding her ski poles. She had a lot of pain in her thumb, which looked swollen.
It sounds like Tess has Skier’s Thumb, an injury to the ulnar collateral ligament of the MCP joint of the thumb.
Mechanism
This injury is usually caused by forced abduction or extension at the MCP joint, typically falling onto an outstretched hand with something in the palm, falling onto an abducted thumb or as a result of a ball or object striking the ulnar aspect of the thumb during sports. This force stretches or tears the ulna collateral ligament, resulting in a complete or partial rupture of the and can be associated with an avulsion fracture.
Presentation
Pain, swelling, and bruising are usually noted over the ulnar aspect (the index finger side) of the MCP joint of the thumb. The patient will also be tender on palpation of this area. Occasionally, a mass or a lump can be felt at the site of tenderness, suggesting a Stener Lesion*. In severe ulnar collateral ligament injuries, the proximal phalanx may become subluxed with radial deviation on the metacarpal head.

*Stener Lesion
-
Normally, the ulnar collateral ligament lies deep to the adductor pollicis tendon.
-
A Sterner Lesion can form when a torn UCL becomes displaced superficially to the adductor pollicis longus.
-
The presence of a Stener Lesion is an indication for surgical repair of this injury.
Evaluation
Evaluation of an ulnar collateral ligament injury involves valgus stress (radial deviation) testing of the joint at neutral and 30 degrees of flexion at the MCP joint of the thumb. Compare the patient’s injured with their uninjured thumb to determine what is normal for that child. Hold the base of the thumb, then apply sideways (lateral) pressure to the tip of the thumb. Increased laxity or lack of an endpoint signifies an injury. It may be kindest to put in a ring block to prevent guarding due to pain to increase the accuracy of the exam.
Functionally, it’s important to test the (in)ability to grasp between thumb and finger. A stable pinch mechanism depends on the integrity of the radial collateral ligament of the index finger and the UCL of the thumb.
An X-ray should be performed to out-rule an avulsion fracture. If an avulsion fracture is present, this will be seen at the ulnar corner of the base of the proximal phalanx. Ultrasound or MRI may be used to identify a tear to the UCL or diagnose the presence of a Stener Lesion.

Treatment
Non-operative: A partial UCL rupture may be treated conservatively. Conservative management involves immobilising the MCP joint in a thumb spica cast or thermoplastic thumb splint.
Operative: Complete UCL rupture or the presence of Stener Lesion are indications for surgical repair. Early immobilization with a thumb spica will also prevent further damage and make it more comfortable for the child while awaiting surgical review.
Tess’ thumb is very bruised and extremely tender. You pop in a ring block, and with valgus stress, you can tell there is increased laxity compared to the other side. There’s no fracture on the x-ray.
You refer Tess to your colleagues in plastics, who, after an ultrasound, diagnose a partial rupture of her ulnar collateral ligament. Her thumb is immobilised in a thumb spica. 6 months later, she’s back on the slopes!

Selected References
Allan, C. H. (2005). Flexor tendons: anatomy and surgical approaches. Hand clinics, 21(2), 151-157.
Armstrong, M. B., & Adeogun, O. (2009). Tendon injuries in the pediatric hand. Journal of Craniofacial Surgery, 20(4), 1005-1010.
Avery, D. M., Inkellis, E. R., & Carlson, M. G. (2017). Thumb collateral ligament injuries in the athlete. Current reviews in musculoskeletal medicine, 10(1), 28-37.
Dorani, B. (2020). Soft Tissue Injuries of the Hand. Retrieved from https://www.rcemlearning.co.uk/reference/soft-tissue-injuries-of-the-hand/#1583314733632-1b04992c-edab
Elson, R. A. (1986). Rupture of the central slip of the extensor hood of the finger. A test for early diagnosis. The Journal of bone and joint surgery. British volume, 68(2), 229-231.
Forward, K. E., Yazdani, A., & Lim, R. (2017). Mallet Finger in a Toddler: A Rare But Easily Missed Injury. Pediatric emergency care, 33(10), e103-e104.
Guly, H.R. (1991). Missed tendon injuries. Archives of Emergency Medicine, (8), 87-91.
Handoll, H. H., & Vaghela, M. V. (2004). Interventions for treating mallet finger injuries. Cochrane Database of Systematic Reviews, (3).
Hatch, D. (2019). Extensor Tendon Injuries. Retrieved from https://www.orthobullets.com/hand/6028/extensor-tendon-injuries
Kalainov, D. M., Hoepfner, P. E., Hartigan, B. J., Carroll IV, C., & Genuario, J. (2005). Nonsurgical treatment of closed mallet finger fractures. The Journal of hand surgery, 30(3), 580-586.
Leggit, J., & Meko, C. J. (2006). Acute finger injuries: part I. Tendons and ligaments. American family physician, 73(5), 810-816.
Lo, I. & Richards, R.S. (1995). Combined Central Slip and Volar Plate Injuries at the PIP Joint. Journal of Hand Surgery, 20B (3), 390-391.
Matzon, J. L., & Bozentka, D. J. (2010). Extensor tendon injuries. The Journal of hand surgery, 35(5), 854-861.
Nugent, N., & O’Shaughnessy, M. (2011). Closed central slip injuries–a missed diagnosis?, Irish Medical Journal, 104 (8):248-250.
Perron, A. D., Brady, W. J., Keats, T. E., & Hersh, R. E. (2001). Orthopedic pitfalls in the emergency department: closed tendon injuries of the hand. The American journal of emergency medicine, 19(1), 76-80.
Ritting, A. W., Baldwin, P. C., & Rodner, C. M. (2010). Ulnar collateral ligament injury of the thumb metacarpophalangeal joint. Clinical Journal of Sport Medicine, 20(2), 106-112.
Shah, A. S., & Bae, D. S. (2012). Management of pediatric trigger thumb and trigger finger. JAAOS-Journal of the American Academy of Orthopaedic Surgeons, 20(4), 206-213.
Sheth, U. (2019). Mallet Finger. Retrieved from https://www.orthobullets.com/hand/6014/mallet-finger
Sullivan, M. A., Cogan, C. J., & Adkinson, J. M. (2016). Pediatric hand injuries. Plastic Surgical Nursing, 36(3), 114-120.
Thurston, M. and Dawes, L. et. al. Gamekeeper Thumb. Retrieved from https://radiopaedia.org/articles/gamekeeper-thumb
Wahba, G., & Cheung, K. (2018). Pediatric hand injuries: Practical approach for primary care physicians. Canadian Family Physician, 64(11), 803-810.
Yoon, A. P., & Chung, K. C. (2019). Management of acute extensor tendon injuries. Clinics in plastic surgery, 46(3), 383-391.
Hi Simon,
Thanks for your feedback! There is a part 1 to this post which covers Seymour fractures. Available at: https://doi.org/10.31440/DFTB.27577
Hi guys,
Excellent well written article!
I just wanted to know if you had considered including a sub-section on Seymour fractures. I know you can’t include every possible hand condition, but this is one I have seen referred as nail plate avulsion with the fracture being missed (it can be very difficult to spot). I always like to give ED clinician’s Seymour’s and Volar plate injuries as ‘sneaky one’s to watch out for’.