

It’s 2am and the crash bleep goes off. You arrive at the bedside of 5-year-old Jerry who has suddenly dropped his sats to 80%. He looks like he has a tracheostomy tube in his neck. Can you keep your cool and handle it like a pro?
Thanks to the team at tracheostomy.org.uk for their support in writing this post. Much of the content is a summary of all the wonderful learning resources on their website and also from their library of videos. This post has been updated in Oct 2020 since it was originally written in 2017. Thanks also to Miran Pankhania (ENT Surgeon in Rotherham, UK) and Eric Levi (ENT Surgeon in Melbourne, Australia) for input.
This update recognises the key differences between paediatric and adult tracheostomy emergency management.
-Paediatric bed signs showing the reasons for the tracheostomy and the type
-Tracheostomies in children are almost all surgical and have stay sutures and maturation sutures which help with emergency management
-In emergency management, have three attempts to change the tube before moving onto oral intubation
-On the third tube reinsertion attempt, use a suction catheter as a guide to insertion.
Do you know the difference between a tracheotomy, a tracheostomy, and a laryngectomy?
Tracheotomy – an incision in the trachea
Tracheostomy – a stoma in the trachea (i.e. an opening which has been created)
Laryngectomy – surgical removal of the larynx – tracheal remnants are stitched to the anterior tracheal wall and there is no connection from the mouth and nose to the rest of the airway. This is almost exclusively an adult procedure though.
Tracheotomy or tracheostomy patients potentially have two airways but a laryngectomy patient only has one.
Which does Jerry have?
It’s very hard to tell by looking at the patient which they have, and hospital inpatients will have a sheet above their bed making it clear which type they have, what pathology they have, and why they have the tracheostomy.
The key things you need to know are:
- is there a connection between their mouth/nose and their lungs? (i.e. 1 or 2 airways)
- are they known to have a difficult airway?
- how old is the tracheostomy and what was the procedure to make it?
A surgical tracheostomy is made by making an incision in the neck and stitching it open – this type of approach will create an established tract. A percutaneous tracheostomy just stretches the skin back to make the stoma and so it more likely to close in 7-10 days if not kept patent.
Why do kids need tracheostomies?
- Bilateral vocal cord palsy with decompensation
- Subglottic or laryngeal stenosis/atresia
- Tracheoesophageal cleft/fistula
- Respiratory toilet and airway protection
- Long term ventilation
- Covering for airway surgery – laryngotracheal reconstruction or as part of EXIT procedure
- Covering for an extra-luminal mass
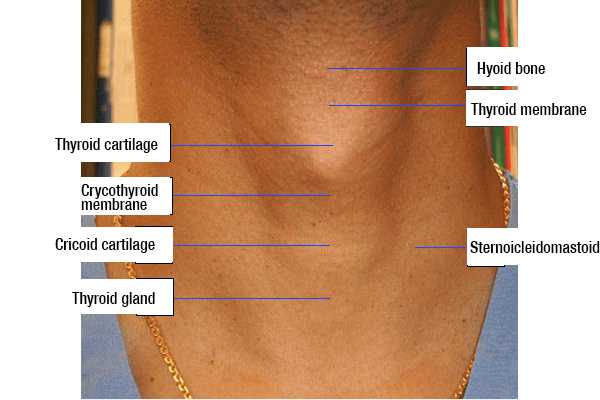
Do you know your anatomy?
Tracheostomy.org.uk has fabulous eLearning resources that goes through the anatomy in more detail. But for now, we can recognise our major landmarks…

{kind=link}

How is a tracheostomy created?
The trachea is entered by making a cut in the anterior tracheal wall at the level of the 2nd or 3rd tracheal cartilage.

Tracheostomies in children are usually open surgical procedures to minimise the risk of hypoxia from accidental decannulation. Whereas tracheostomies in adults are usually percutaneous procedures.
The child’s neck is fatty by comparison to an adult neck, so the subcutaneous fat is often removed to make the trachea as close to the skin as possible in the event of accidental decannulation.
Stay sutures are put in the tracheal wall (akin to parachute cords) to bring the tracheotomy to the skin and open it in case of decannulation.
Maturation sutures are from the tracheotomy to the skin to align all the holes made and minimise risk from decannulation and facilitate re-intubation of the stoma.

What could have gone wrong with Jerry’s tracheostomy?
Complications of tracheostomies are split into peri-operative, early postoperative, and late post-operative
Peri-operative: haemorrhage; misplaced tube; pneumothorax; tube occlusion; surgical emphysema
Early post-operative (<7 days): tube blockage; tube displacement; site infection; lung infection; tracheal ulceration; fistula; haemorrhage
Late post-operative (>7 days): granuloma; tracheal collapse; blocked tube; haemorrhage; tracheal stenosis
What are the different types of tubes?
Shiley do Neo and Ped trachy tubes are the main types. These are single lumen plus or minus a cuff (depending on the indication for insertion).
Paediatric tracheostomy tubes are usually uncuffed with no inner tube. This is because the trachea has a small diameter, and an inner tube would reduce that even further. Cuffed tubes can be used in cases where high pressures are needed or these is a risk of aspiration.
If a patient has an uncuffed tube, that patient has no airway protection from aspiration, but air can flow through the mouth and nose and down past the tube.

If a patient has a cuffed tube, that patient’s airway is protected from aspiration, but the tracheostomy is the only route for airflow (which is a problem if the tube becomes blocked). If you deflate the cuff, air can flow from the mouth and nose down the trachea.

Tracheostomy tubes come with lots of different additions. Most of these are Heat-Moisture Exchanges e.g. the Swedish nose. These help maintain humidity (like a real nose). During normal breathing, air is warmed, filtered and moistened by ciliated epithelial cells in the nose and upper airways. However, this does happen with a tracheostomy tube and so air inspired will be cold and dry. The HMEs conserve heat and moisture on expiration.
Now we have a good understanding of the anatomy and types of tracheostomies, how are we going to help Jerry?
Follow a step-by-step approach to managing tracheostomy emergencies.
1. Call for help (anaesthetics or ENT).
Establish how many airways we have to work with. Has Jerry had a laryngectomy (one airway) or a tracheostomy (two airways)? Look for a sign around his bed.

2. Look, listen, and feel at the mouth and the stoma.
Is the patient breathing? If not then consider airway positioning (depending on the age of the child).
In real life, many time where there are desaturations and difficulty ventilating, it is due to either clots or mucous plugging, or due to positioning (i.e. tracheostomy tube is too short and ends up hitting back wall of trachea, or too long and ends up in one bronchi). Extending the neck/shoulder roll and suctioning the tube vigorously may help resolve lots of common obstruction.
Jerry is breathing, but if he wasn’t we would check a pulse and follow the APLS algorithm. He has a tracheostomy with an uncuffed tube.
3. Apply high flow oxygen
Apply to the mouth and nose (if the patient has two airways, which we now know Jerry does) and to the tracheostomy. This will require two oxygen sources.

Then think about some common tracheostomy problems:
- Remove any attachments e.g. speaking valve or caps
- Remove the inner cannula if there is one (although not common in younger children)
- Assess patency by putting a suction catheter down (this is better than just bagging first because if the tube is dislodged you will cause surgical emphysema by bagging). If you can pass the catheter then you should suction and ventilate if they are not breathing.
You try to pass a suction catheter down Jerry’s tube, but you cannot pass it.
If you can’t pass the catheter then the problem is that the tracheostomy is blocked and it’s time to problem solve.
4. Do an emergency tracheostomy tube change
Jerry needs and emergency tube change. This is a key difference in children as Jerry will have maturation sutures – so this should be attempted before upper airway management. You need to cut and remove any tapes and aim for immediate reinsertion. If there are stay sutures then lift them up and out by hand.
Try to put one of the same size in again. No bougie, wire or catheter is recommended. An obturator can help guide insertion and protect the stoma. If it goes back in then check it is patent and assess again by look, listening, and feeling at the tracheostomy and mouth/nose (and reapply oxygen). Some gentle ventilation can be attempted if there are no spontaneous respiration efforts. Don’t attempt to ventilate if the suction catheter won’t pass – you do not want to cause subcutaneous emphysema if the tube is in a false passage.
5. Try a second emergency tracheostomy tube change
Try again with a tube a half-size smaller. Consider changing the position of the child to bring the trachea anteriorly.
Try oral airway manoeuvres by covering the stoma with gauze or your hand and: bag-valve-mask; oral or nasal airway adjuncts; or an LMA.
6. Try a third emergency tracheostomy tube change with a suction catheter
If this second attempt doesn’t work, then try a third attempt. This time use a soft suction catheter as a guide for your tube to go over (like the Seldinger technique). Also use a half size smaller than the original tube (same size as the second attempt).
You have removed the tracheostomy tube but Jerry is still not breathing (he has a pulse). You cannot replace the tube on your first three attempts.
7. Go for emergency oxygenation
Try oxygenation with the mouth (via bag-valve mask) or with a supraglottic airway. If this isn’t working then try via the stoma with a bag-valve mask over the stoma, or an LMA over the stoma.

If you aren’t able to ventilate Jerry with these basic maneouvres. It’s time for something more invasive.
8. Attempt oral intubation
Attempt oral intubation, but prepare for a difficult intubation and make sure your ETT passes the stoma.
9. Attempt intubation of the stoma
Attempt intubation of the stoma itself using a tracheal tube a half-size smaller than the previous tube. There is a risk of blindly intubating a stoma as you may create a false tract. If you have someone (or are someone) with more experience, you can put your finger into the trachea and guide the bougie, or use a fibre-optic technique.
10. This is a CICO situation
At this point you need to declare a CICO. Attempts should be made by more experienced staff, or emergency front of neck access will be required. Remember though that a tracheostomy is the quintessential FONA. If the tracheostomy tube fails, either a significant false passage, complete obstruction, or distal pathology at the level of the carina & bronchi has occurred. Definitive means to salvage this situation is tricky and may involve the urgent use of a flexible or rigid tracheobronchoscopic assessment to visualise the distal pathology.
Thankfully using a face mask over the stoma works and Jerry picks up just as the Anaesthetic Consultant arrives.
If you want a nice summary with Sheila rather than Jerry – then watch this fabulous video of the emergency tracheostomy algorithm.
Selected references:
The Association of Anaesthetists of Great Britain & Ireland grants readers the right to reproduce the algorithms included in this article (Figs 1 and 2) for non-commercial purposes (including in scholarly journals, books and non-commercial websites), without the need to request permission. Each reproduction of any algorithm must be accompanied by the following text: Reproduced from McGrath BA, Bates L, Atkinson D, Moore JA. Multidisciplinary guidelines for the management of tracheostomy and laryngectomy airway emergencies. Anaesthesia. 2012 Jun 26. doi: 10.1111/j.1365-2044.2012.07217, with permission from the Association of Anaesthetists of Great Britain & Ireland/Blackwell Publishing Ltd.
Check out tracheostomy.org.uk for more resources on this topic and read the paediatric tracheostomy emergencies guideline here: https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/full/10.1111/anae.14307
Thanks so much for this concise and clear update. I am thankful to my colleague Liz Herrieven who signposted this to me. Many thanks to the entire DFTB team.
Tnxx 100%
Thanks for the advice to figure out how many airways you have to work with after calling for help. My dad has been having trouble breathing lately, so I want to be prepared for any instance if something were to happen. When it comes to a tracheostomy, I will definitely find a professional in my area who we can work with in the case of an emergency.